Non-Germinomatous Germ Cell Tumour¶
Summary
- Rare intracranial neoplasms arising from primordial germ cells
- Heterogeneous group including teratomas, embryonal carcinomas, yolk sac tumours, and choriocarcinomas
- Typically present with mass effect symptoms and have variable imaging appearances
Pathophysiology¶
- Arise from primordial germ cells that fail to migrate properly during embryogenesis
- Classified based on histological components:
- Teratoma: contains tissue from all three germ layers
- Embryonal carcinoma: undifferentiated cells resembling embryonic stem cells
- Yolk sac tumour: endodermal sinus-like structures
- Choriocarcinoma: trophoblastic differentiation
- Often mixed tumours with multiple histological components
Demographics¶
- Rare, accounting for <5% of all primary intracranial tumours
- Peak incidence in adolescents and young adults (10-21 years)
- Male predominance (M:F ratio 2-3:1)
- Most common locations:
- Pineal region
- Suprasellar region
- Basal ganglia/thalamus
Diagnosis¶
- Clinical presentation:
- Mass effect symptoms (headache, nausea, vomiting)
- Visual disturbances (if suprasellar)
- Endocrine dysfunction
- Precocious puberty (in some cases)
- Tumour markers:
- Alpha-fetoprotein (AFP)
- Beta-human chorionic gonadotropin (β-hCG)
- Placental alkaline phosphatase (PLAP)
- Cerebrospinal fluid (CSF) cytology for staging
Imaging¶
- CT:
- Heterogeneous mass with variable enhancement
- Calcifications common in teratomas
- MRI:
- T1: Variable signal intensity
- T2: Heterogeneous, often hyperintense
- T1 post-contrast: Heterogeneous enhancement
- DWI: Variable restriction
- Susceptibility-weighted imaging (SWI): May show haemorrhage or calcifications
- Specific features:
- Teratoma: Fat-containing components, calcifications
- Embryonal carcinoma: Large, heterogeneous masses with necrosis and haemorrhage
- Yolk sac tumour: Cystic components, haemorrhage
- Choriocarcinoma: Haemorrhagic mass
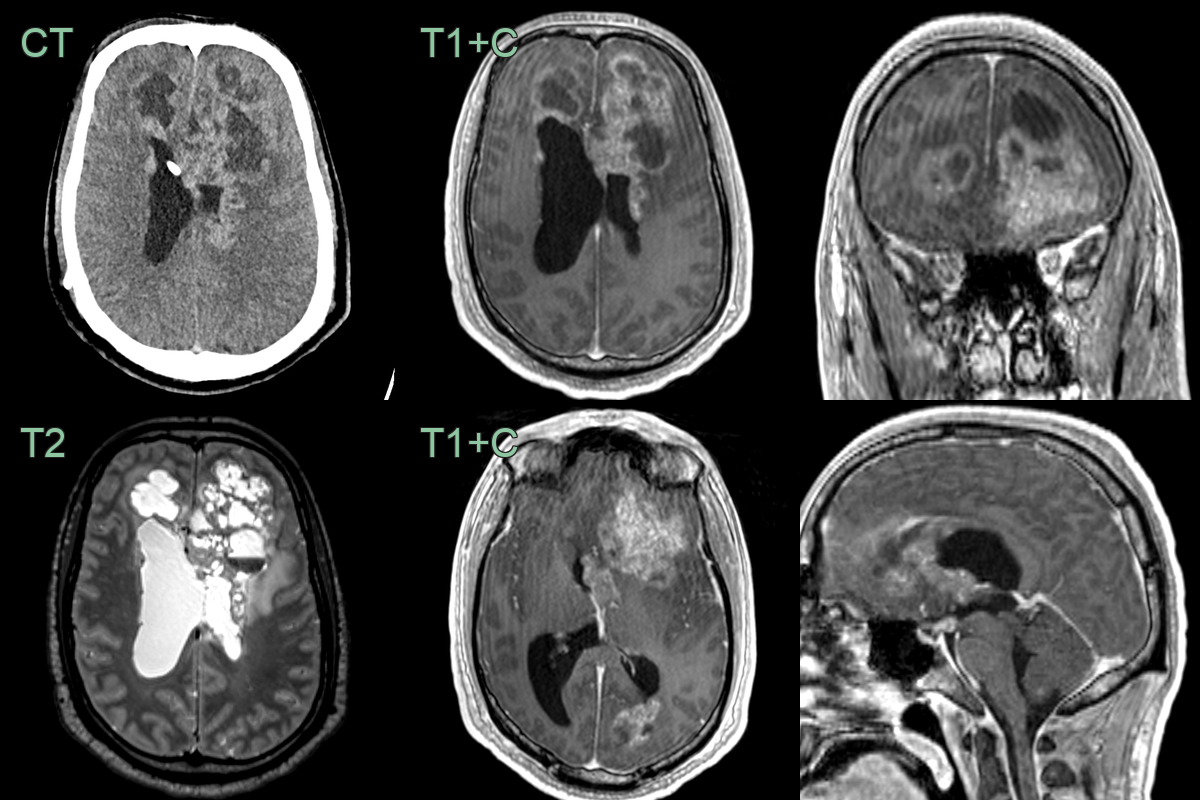
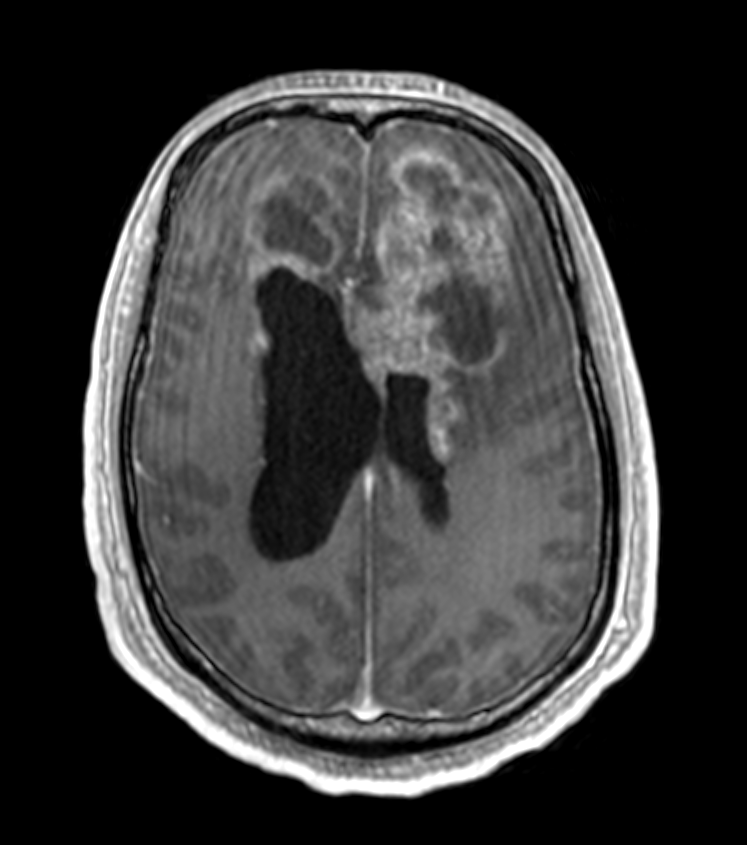
- A 25-year-old patient presented with headache, lethargy, and various neurological deficits.
- CT showed hydrocephalus secondary to a large hyperdense solid-cystic lesion.
- The lesion was enhancing and contained fluid-fluid levels and petechial haemorrhage based on SWI (not shown). The lesion extended along the ependyma and involved the infundibulum.
- The final diagnosis was a non-germinomatous germ cell tumour.
Treatment¶
- Multimodal approach:
- Surgery: Maximal safe resection
- Chemotherapy: Platinum-based regimens (e.g., cisplatin, etoposide)
- Radiotherapy: Craniospinal irradiation for disseminated disease
- Risk-adapted treatment based on histology and tumour markers
- Regular follow-up imaging and tumour marker monitoring
- Overall prognosis poorer than germinomas, but varies by histological subtype
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Germinoma | Typically has a more homogeneous appearance on imaging; better prognosis |
| Pineoblastoma | Usually occurs in younger patients; more aggressive behaviour |
| Ependymoma | Tends to have a more well-defined margin; often enhances more uniformly |
| Choroid plexus papilloma | Usually located within ventricles; tends to be more vascular |
| Craniopharyngioma | Often contains calcifications; cystic components more common |
| Metastasis | Multiple lesions at grey-white junction; no pineal or suprasellar predilection; no fat or calcification |
| Lymphoma | Tends to be more homogeneous; often shows restricted diffusion on MRI |
| Teratoma | May contain fat, calcifications, or teeth; more heterogeneous appearance |
| Astrocytoma | Usually lacks markers like AFP or β-hCG; different cellular origin |
| Pineal parenchymal tumour | Typically arises from pineal gland; different cellular origin |