Normal Pressure Hydrocephalus¶
Summary
- Chronic communicating hydrocephalus characterised by the clinical triad of gait disturbance, urinary incontinence, and cognitive decline
- Enlarged ventricles with normal intracranial pressure and preserved brain parenchyma
- Potentially reversible cause of dementia, treatable with cerebrospinal fluid (CSF) diversion
Pathophysiology¶
- Impaired CSF absorption and/or altered CSF dynamics
- Possible mechanisms:
- Reduced compliance of subarachnoid space
- Increased resistance to CSF outflow
- Altered brain viscoelasticity
- Ventricular enlargement leads to stretching of periventricular white matter tracts
Demographics¶
- Typically affects adults over 60 years of age
- Estimated prevalence: 0.5-2.9% in individuals aged 65 and older
- Male to female ratio approximately 1.5:1
- Risk factors:
- Advanced age
- Cerebrovascular disease
- Hypertension
- Diabetes mellitus
Diagnosis¶
- Clinical triad:
- Gait disturbance: broad-based, shuffling, "magnetic" gait
- Urinary incontinence: urgency, frequency, or frank incontinence
- Cognitive decline: executive dysfunction, psychomotor slowing
- Supplementary tests:
- CSF tap test: improvement in gait after large-volume CSF removal
- Lumbar drainage: extended CSF drainage over 2-3 days
- Intracranial pressure monitoring
Imaging¶
- CT:
- Ventriculomegaly (Evans' index >0.3)
- Periventricular hypodensity
- Effaced sulci at high convexity/midline
- MRI:
- T1-weighted: enlarged ventricles
- T2-weighted/FLAIR: periventricular hyperintensities
- Flow void sign in aqueduct on T2-weighted images
- Disproportionately enlarged subarachnoid space hydrocephalus (DESH)
- Cisternography:
- Delayed clearance of radioisotope from ventricles
- Phase-contrast MRI:
- Altered CSF flow dynamics in aqueduct
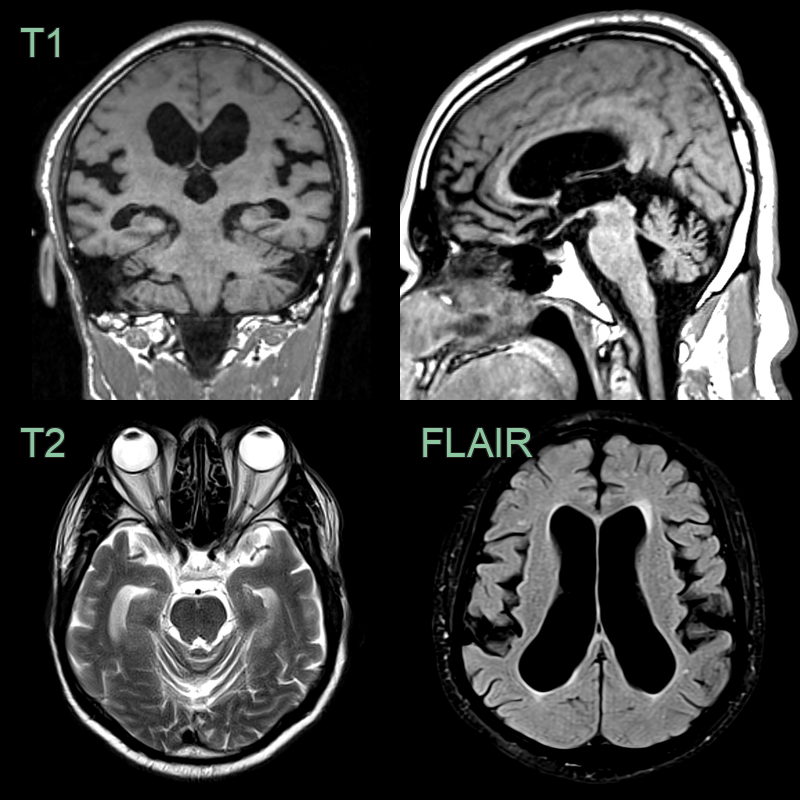
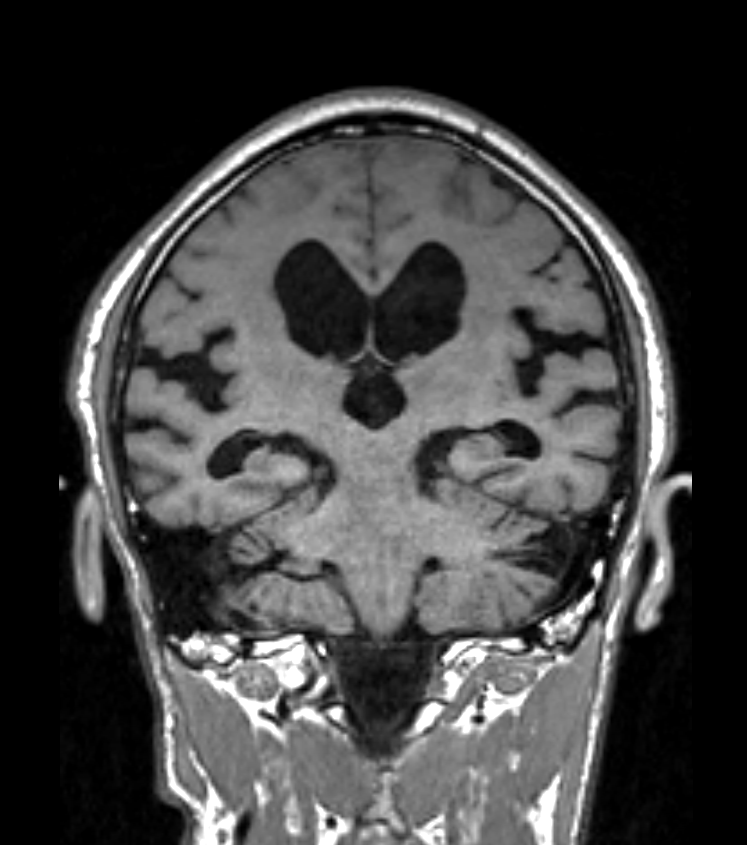
- 70-year-old patient presented with poor balance and sphincter disturbance.
- MRI showed ventriculomegaly, an acute callosal angle, widening of the Sylvian fissures, crowding at the vertex, upward bowing of the corpus callosum, progressive anterior-posterior narrowing of the cingulate fissure.
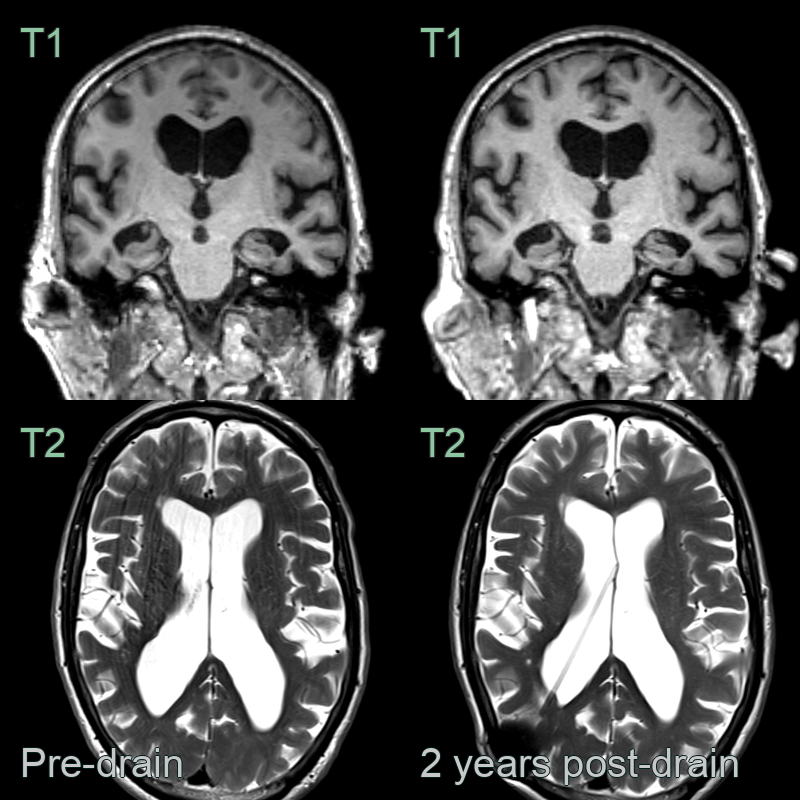
- A 75-year-old patient presented with memory issues and a shuffling gait.
- MRI showed ventriculomegaly, disproportionate enlargement of the sylvian fissures, and effacement of sulci at the vertex.
- 2 years following shunt insertion, the widening of the sylvian fissures and the effacement of sulci at the vertex improved.
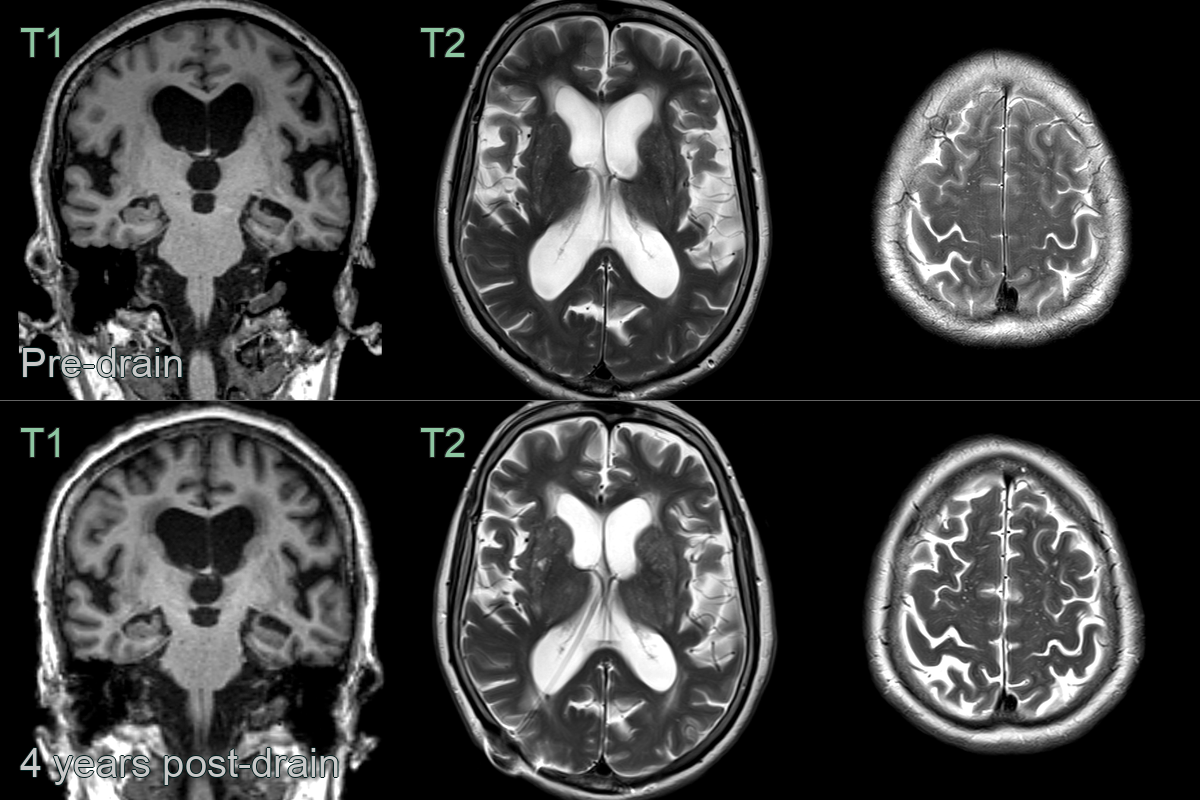
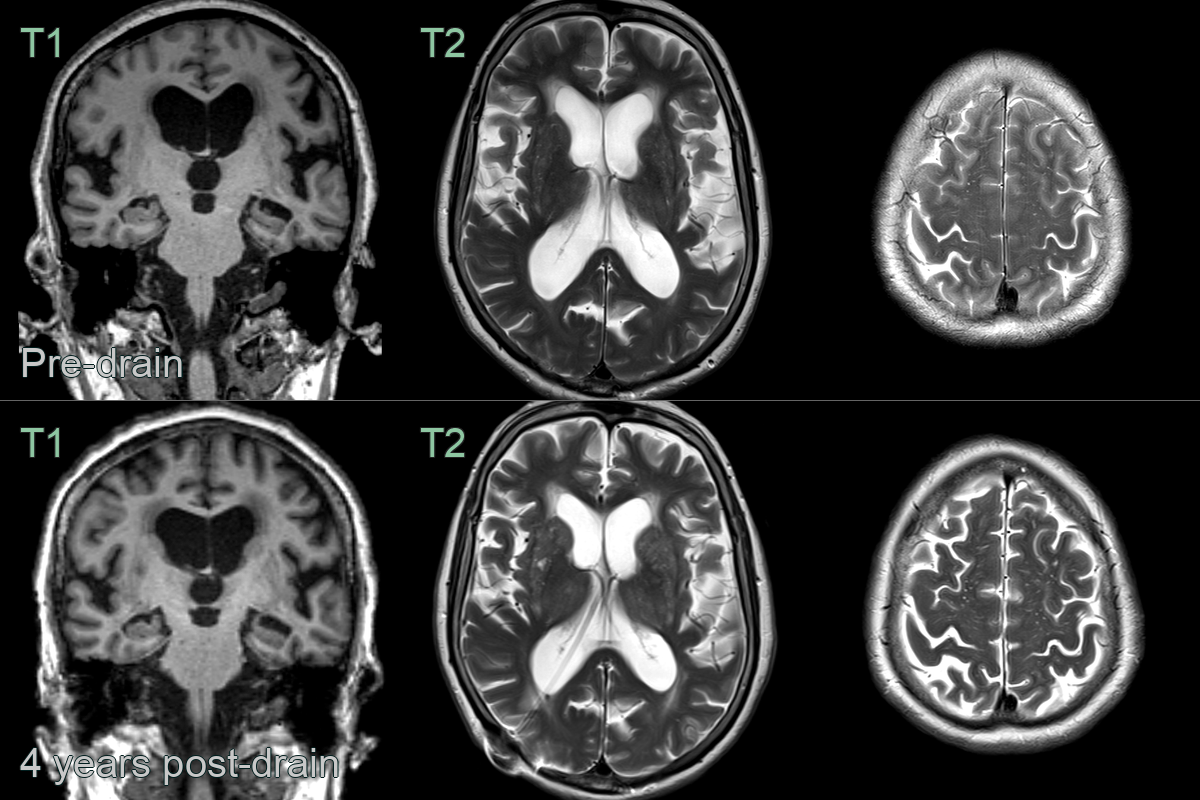
- An 80-year-old patient presented with progressive gait and cognitive syndrome.
- Four years after the insertion of a shunt, effacement of sulci at the vertex and the widening of the sylvian fissures improved.
- A 70 year old presented with cognitive impairment and a broad based gait.
- MRI showed ventriculomegaly, focally expanded sulci, upward bowing of the corpus callosum, narrowed callosal angle, widening of the sylvian fissures.
- The patient had a remarkable response to a diagnostic lumbar drain and was subsequently shunted.
Treatment¶
- CSF diversion:
- Ventriculoperitoneal (VP) shunt: most common
- Lumboperitoneal (LP) shunt: alternative option
- Endoscopic third ventriculostomy: in selected cases
- Shunt valve selection:
- Programmable valves allow post-operative pressure adjustments
- Gravitational valves may reduce overdrainage complications
- Complications:
- Shunt malfunction
- Infection
- Subdural haematoma
- Over-drainage syndrome
- Post-operative management:
- Regular clinical follow-up
- Imaging to assess ventricular size and shunt position
- Shunt valve pressure adjustments as needed
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Cerebral atrophy (ex vacuo ventriculomegaly) | Ventricular enlargement proportional to sulcal widening; no DESH pattern; absent CSF flow void |
| Obstructive hydrocephalus | Dilatation of ventricles proximal to an obstruction; aqueductal stenosis or mass visible |