Optic Nerve Glioma¶
Summary

- Benign, slow-growing tumour of the optic pathway, most commonly pilocytic astrocytoma (WHO grade 1), predominantly affecting children
- Strong association with neurofibromatosis type 1 (NF1), presenting with progressive vision loss, proptosis, and optic nerve enlargement
- MRI demonstrates fusiform optic nerve enlargement with variable enhancement and characteristic "kinked" appearance when involving the optic nerve
Pathophysiology¶
- Most commonly pilocytic astrocytoma (WHO grade 1)
- Composed of bipolar cells with Rosenthal fibres and eosinophilic granular bodies
- BRAF-KIAA1549 fusion or BRAF V600E mutations common in sporadic cases
- Arise from astrocytes within the optic nerve, chiasm, or optic tracts
- Can extend along the visual pathway:
- Anterior: intraorbital optic nerve
- Posterior: optic chiasm, optic tracts, optic radiations
- Growth patterns:
- Intrinsic: expansion within nerve sheath
- Exophytic: growth beyond nerve sheath
- Perineural: arachnoidal gliomatosis (rare)
Demographics¶
- Peak incidence: 4-6 years of age
- 90% occur before age 20
- Slight female predominance (1.2:1)
- Strong association with NF1:
- 15-20% of NF1 patients develop optic pathway gliomas
- 10-70% of optic pathway gliomas occur in NF1 patients
- Bilateral optic nerve gliomas almost pathognomonic for NF1
- Better prognosis in NF1-associated cases (often indolent course)
Diagnosis¶
- Clinical presentation:
- Progressive vision loss (most common)
- Proptosis (especially with intraorbital involvement)
- Strabismus
- Nystagmus (chiasmal involvement)
- Optic disc swelling or atrophy
- Precocious puberty (hypothalamic involvement)
- Visual field testing: variable defects depending on location
- Fundoscopy: optic disc oedema, pallor, or atrophy
- Biopsy rarely performed due to risk of vision loss
- Diagnosis typically based on imaging in appropriate clinical context
Imaging¶
- MRI (modality of choice):
- T1: isointense to hypointense relative to gray matter
- T2: hyperintense with fusiform or tubular enlargement of optic nerve
- T1+C: variable enhancement (typically avid but can be minimal or absent)
- DWI: usually no restricted diffusion (helps differentiate from malignant gliomas)
- STIR: hyperintense, useful for orbital imaging
- Fat-suppressed T1+C: optimal for evaluating orbital and intracanalicular segments
- Imaging patterns:
- Fusiform enlargement with "kinked" or buckled appearance
- Smooth tubular thickening
- Globular or exophytic masses (chiasmal/hypothalamic involvement)
- "Pseudo-CSF" sign: peripheral hyperintense cystic areas on T2
- CT findings:
- Iso- to hyperdense tubular enlargement
- Optic canal expansion (chronic cases)
- Calcification rare
- Additional findings in NF1:
- Unidentified bright objects (UBOs) in basal ganglia, brainstem, cerebellum
- Plexiform neurofibromas
- Sphenoid wing dysplasia
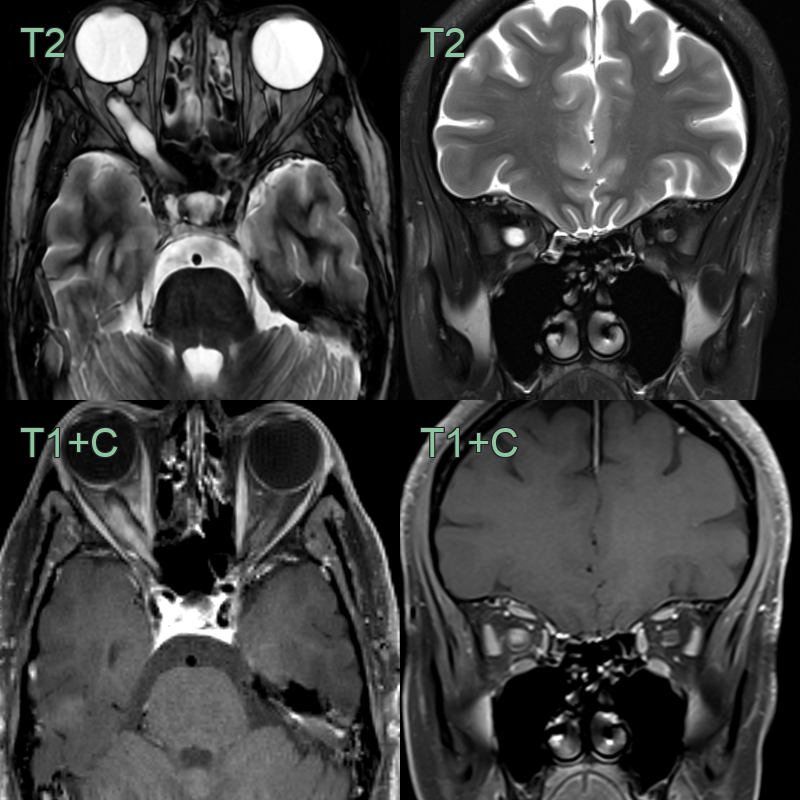
- A 40-year-old patient presented with a visual field defect and optic nerve swelling that was identified by an optician.
- Imaging showed a thickened and hyperintense optic nerve with patchy enhancement.
Treatment¶
- Observation:
- First-line for stable, asymptomatic lesions
- Regular ophthalmologic and MRI surveillance
- Particularly in NF1 patients (often spontaneous stabilization)
- Chemotherapy:
- First-line for progressive or symptomatic disease
- Carboplatin/vincristine (standard regimen)
- Alternative agents: vinblastine, bevacizumab
- Better response in younger patients
- Radiation therapy:
- Reserved for refractory cases
- Avoided in N
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Optic nerve sheath meningioma | Peripheral "tram-track" or "doughnut" enhancement; nerve itself spared centrally; calcifications common; optic canal wall thickening |
| Optic neuritis | Enhancement of nerve without fusiform enlargement; no mass effect; resolves on follow-up |