Optic Nerve Sheath Meningioma¶
Summary

- Rare benign tumour arising from meningothelial cells of the optic nerve sheath
- Typically presents with gradual, painless vision loss and proptosis
- Characteristic "tram-track" sign on contrast-enhanced imaging
Pathophysiology¶
- Originates from arachnoid cap cells within the optic nerve sheath
- Grows circumferentially around the optic nerve, causing compression
- May extend intracranially through the optic canal
- Histologically similar to intracranial meningiomas
Demographics¶
- Accounts for 1-2% of all orbital tumours
- Female predominance (3:1 female to male ratio)
- Peak incidence in middle-aged adults (30-50 years)
- Rare in children, but associated with neurofibromatosis type 2 when present
Diagnosis¶
- Clinical presentation:
- Gradual, painless monocular vision loss
- Proptosis
- Optic disc oedema or atrophy
- Optociliary shunt vessels (in advanced cases)
- Ophthalmologic examination:
- Visual acuity testing
- Visual field testing (typically central or arcuate defects)
- Fundoscopy
- Diagnostic criteria:
- Characteristic imaging findings
- Clinical presentation
- Exclusion of other orbital masses
Imaging¶
- CT:
- Fusiform enlargement of the optic nerve
- Calcifications in 20-25% of cases
- Hyperostosis of adjacent bone (uncommon)
- MRI:
- T1: Isointense to slightly hypointense to brain
- T2: Variable signal intensity
- T1 post-contrast:
- "Tram-track" sign: Circumferential enhancement around a non-enhancing central optic nerve
- "Doughnut" sign on axial images
- Fat-suppressed sequences helpful for delineating tumour extent
- Differential diagnosis:
- Optic nerve glioma
- Orbital pseudotumour
- Sarcoidosis
- Metastases
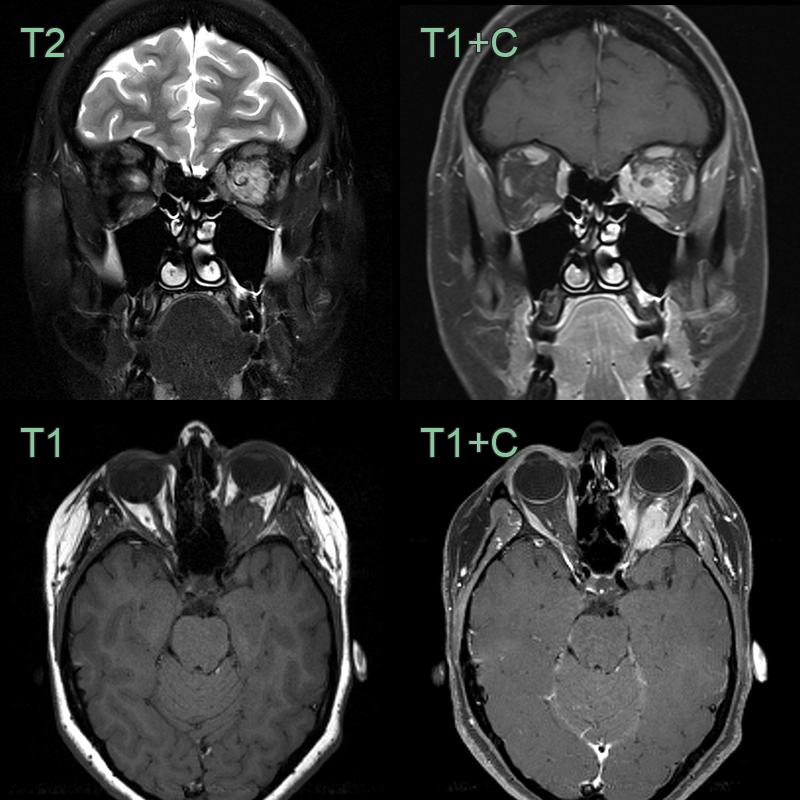
- 40-year-old patient presenting with left sided proptosis.
- MRI showed an avidly enhancing lesion filling the orbital apex and encasing the optic nerve.
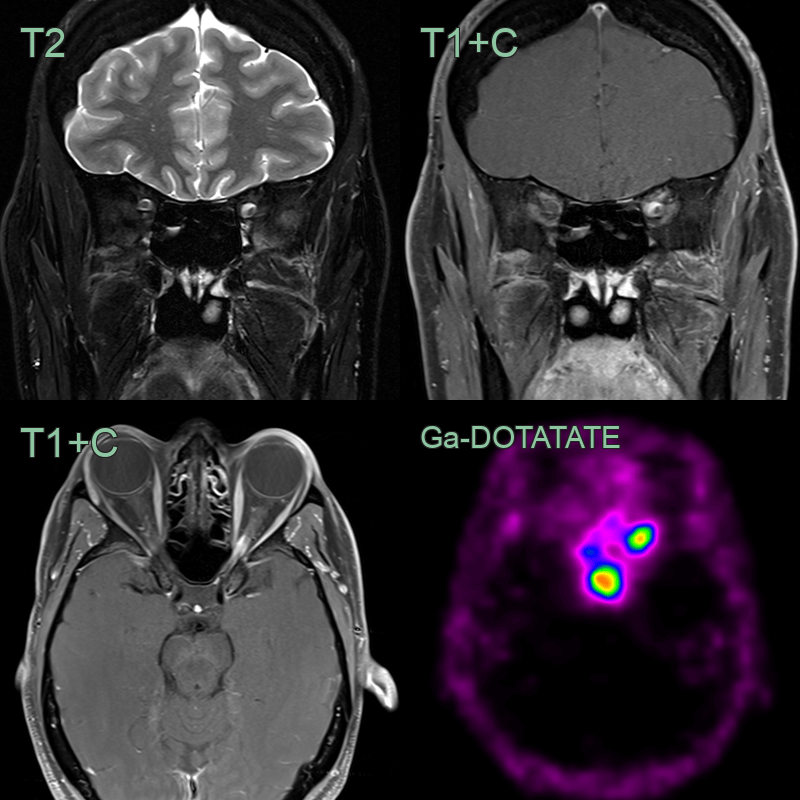
- 45-year-old female with eccentric enhancement of the left optic nerve sheath near the orbital apex.
- There was very high uptake on the Ga-DOTATATE PET scan.
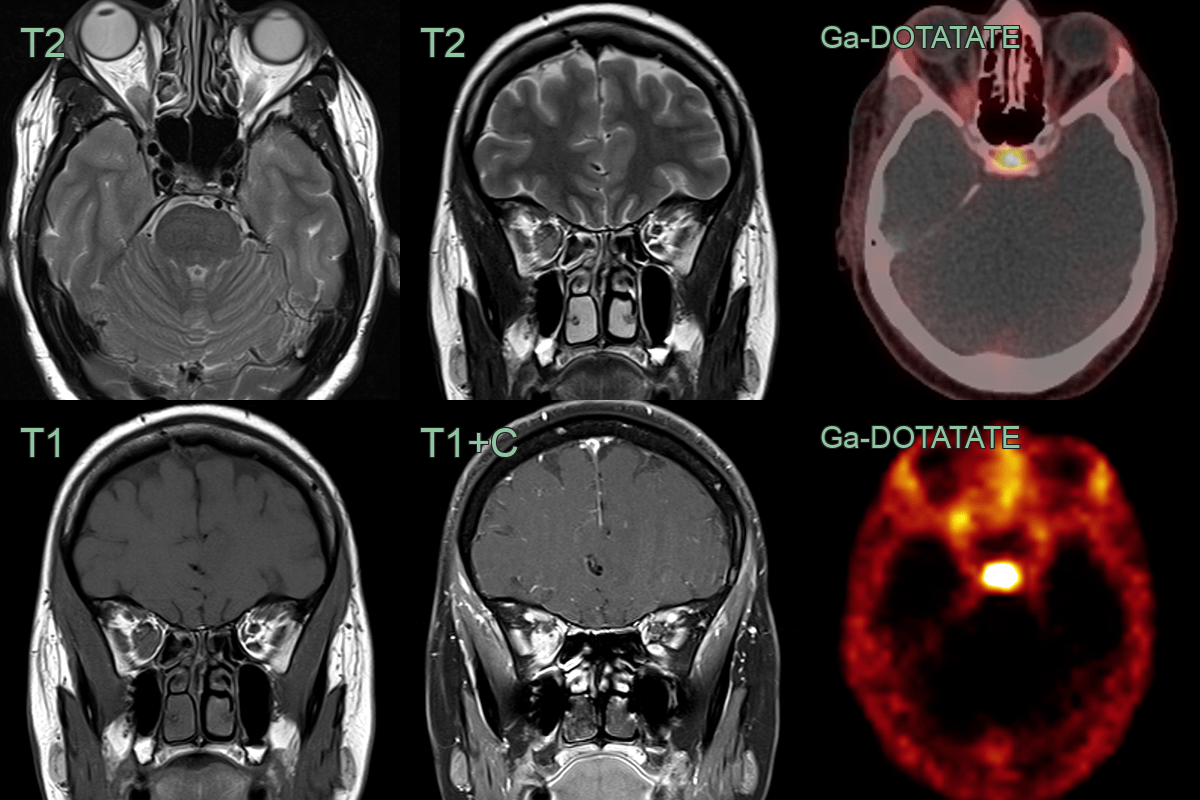
- 35-year-old patient developed worsening orbital swelling during pregnancy.
- An enhancing mass lesion along the inferior aspect of the optic nerve sheath, causing 2 mm of proptosis, was avid on Ga-DOTATATE PET.
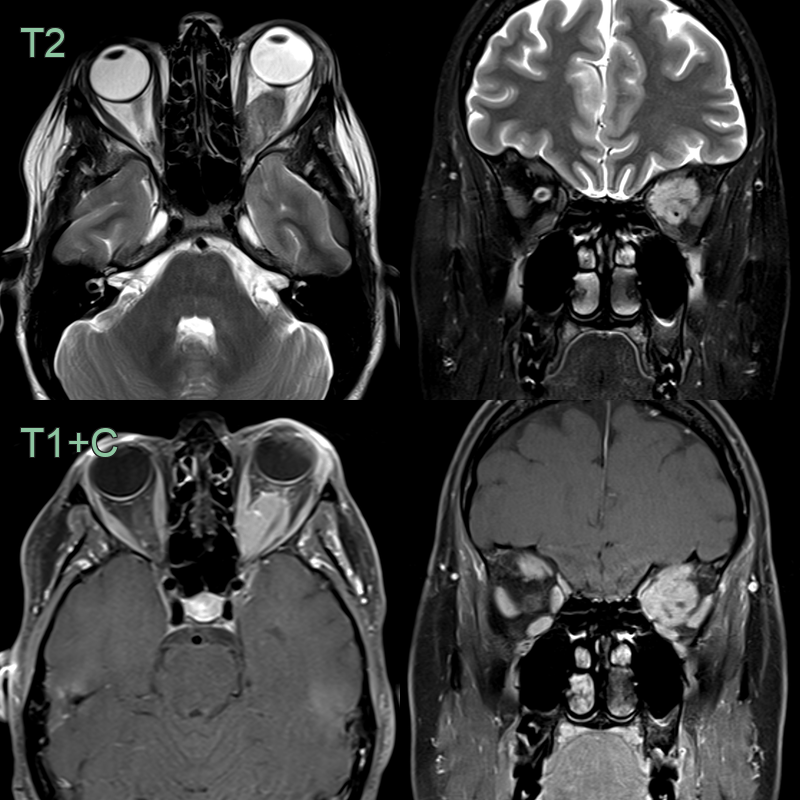
- 30-year-old patient presented with proptosis but no visual symptoms.
- MRI showed proptosis secondary to a large enhancing lesion encasing the optic nerve (red arrow).
Treatment¶
- Observation for small, asymptomatic tumours
- Fractionated stereotactic radiotherapy:
- First-line treatment for most cases
- Aims to halt tumour growth and preserve vision
- Surgery:
- Reserved for large tumours with significant proptosis or intracranial extension
- Risk of complete vision loss in the affected eye
- Systemic therapy:
- Limited role
- Hydroxyurea or temozolomide may be considered in select cases
- Follow-up:
- Regular ophthalmologic examinations
- Periodic MRI to monitor tumour size and extension
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Optic nerve glioma | Intrinsic fusiform enlargement of the nerve itself; no peripheral tram-track enhancement; calcification absent |
| Orbital pseudotumour | Diffuse infiltration of orbital fat and extraocular muscles; no discrete encasing mass; variable enhancement |
| Orbital lymphoma | Homogeneous soft tissue mass moulding to orbital structures; no calcification; may involve lacrimal gland |
| Orbital metastases | Known primary malignancy; irregular margins; bone destruction in aggressive types |
| Sarcoidosis | Enhancing optic nerve with leptomeningeal spread; bilateral optic nerve involvement; no tram-track sign |