Optic Pathway Glioma¶
Summary
- Optic pathway gliomas (OPGs) are low-grade astrocytomas affecting the optic nerves, chiasm, and/or optic tracts
- Commonly associated with neurofibromatosis type 1 (NF1)
- Typically present in childhood with visual disturbances, proptosis, or endocrine dysfunction
Pathophysiology¶
- Arise from glial cells (primarily astrocytes) of the optic pathway
- WHO grade 1 pilocytic astrocytomas in most cases
- May involve:
- Optic nerves
- Optic chiasm
- Optic tracts
- Hypothalamus (in some cases)
- Associated with NF1 mutations in about 30% of cases
Demographics¶
- Most common in children, with 75% diagnosed before age 10
- Accounts for 3-5% of all paediatric brain tumours
- Slightly higher incidence in females
- 15-20% of NF1 patients develop OPGs
Diagnosis¶
- Clinical presentation:
- Visual disturbances (decreased acuity, visual field defects)
- Proptosis
- Strabismus
- Nystagmus
- Endocrine dysfunction (if hypothalamic involvement)
- Ophthalmologic examination:
- Optic disc pallor or swelling
- Visual field testing
- Endocrine evaluation if hypothalamic involvement suspected
Imaging¶
- MRI is the imaging modality of choice
- T1-weighted: Iso- to hypointense
- T2-weighted: Hyperintense
- FLAIR: Hyperintense
- T1 post-contrast: Variable enhancement patterns
- CT:
- Hypodense or isodense masses
- Calcifications uncommon
- Key imaging features:
- Fusiform enlargement of optic nerves
- "Dotted i" sign: chiasmatic involvement with posterior extension
- Hypothalamic involvement may appear as a suprasellar mass
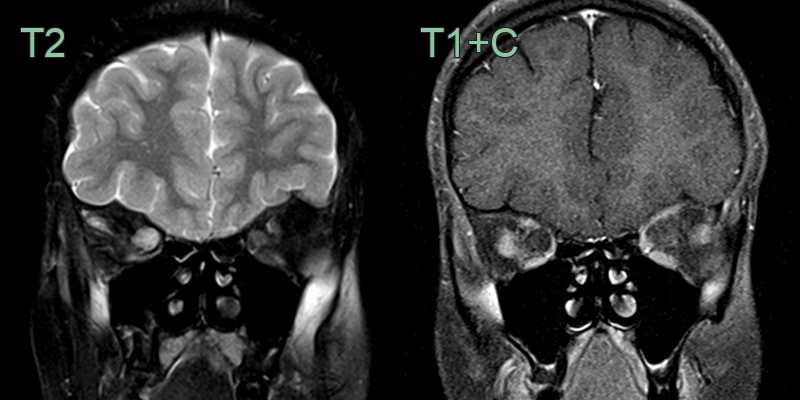
- A right sided orbital optic nerve glioma caused fusiform dilatation and hyperintensity of the optic nerve without enhancement.
Treatment¶
- Management depends on:
- Tumour location and extent
- Presence of NF1
- Visual function
- Rate of progression
- Options include:
- Observation with serial imaging and ophthalmologic exams
- Chemotherapy:
- First-line for most paediatric cases
- Carboplatin-based regimens common
- Surgery:
- Limited role due to risk of visual loss
- May be considered for large chiasmatic/hypothalamic tumours causing mass effect
- Radiation therapy:
- Generally avoided in young children due to long-term sequelae
- May be considered in older children or adults with progressive disease
- Prognosis:
- Generally favourable, with 5-year progression-free survival >90%
- NF1-associated OPGs tend to have a more indolent course
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Optic neuritis | Acute onset, pain with eye movement, often unilateral |
| Craniopharyngioma | Calcifications on imaging, suprasellar location |
| Meningioma | Dural tail sign on MRI; peripheral "tram-track" pattern; intracranial extension along dura |
| Pituitary adenoma | Sellar location; suprasellar extension compressing chiasm from below; no intrinsic nerve enlargement |
| Optic nerve sheath meningioma | "Tram-track" enhancement on CT; nerve spared centrally; calcifications |
| Optic neuritis | Enhancement of nerve without fusiform enlargement; no mass effect; resolves on follow-up |
| Multiple sclerosis | Short T2 signal in optic nerve without mass effect; periventricular brain lesions; Dawson's fingers |
| Langerhans cell histiocytosis | Lytic calvarial or orbital bone lesions; infundibular thickening; diabetes insipidus on MRI |
| Orbital lymphoma | Homogeneous enhancing mass moulding around orbital structures; no tubular nerve enlargement |