Ossification of the Falx Cerebri¶
Summary
- Rare condition characterised by calcification or ossification of the falx cerebri
- Typically asymptomatic and discovered incidentally on imaging
- May be associated with underlying metabolic disorders or age-related changes
Pathophysiology¶
- Exact mechanism unclear, but proposed theories include:
- Dystrophic calcification due to chronic inflammation or microtrauma
- Metaplastic bone formation in dural connective tissue
- Abnormal calcium metabolism in some cases
Demographics¶
- Prevalence increases with age, more common in elderly population
- No significant gender predilection reported
- Rare in children, but cases have been documented
- Higher prevalence in certain ethnic groups (e.g., Japanese)
Diagnosis¶
- Often an incidental finding on neuroimaging studies
- Clinical presentation:
- Usually asymptomatic
- Rarely associated with headaches or seizures
- Differential diagnosis:
- Meningioma
- Dural metastases
- Intracranial calcifications of other aetiologies
Imaging¶
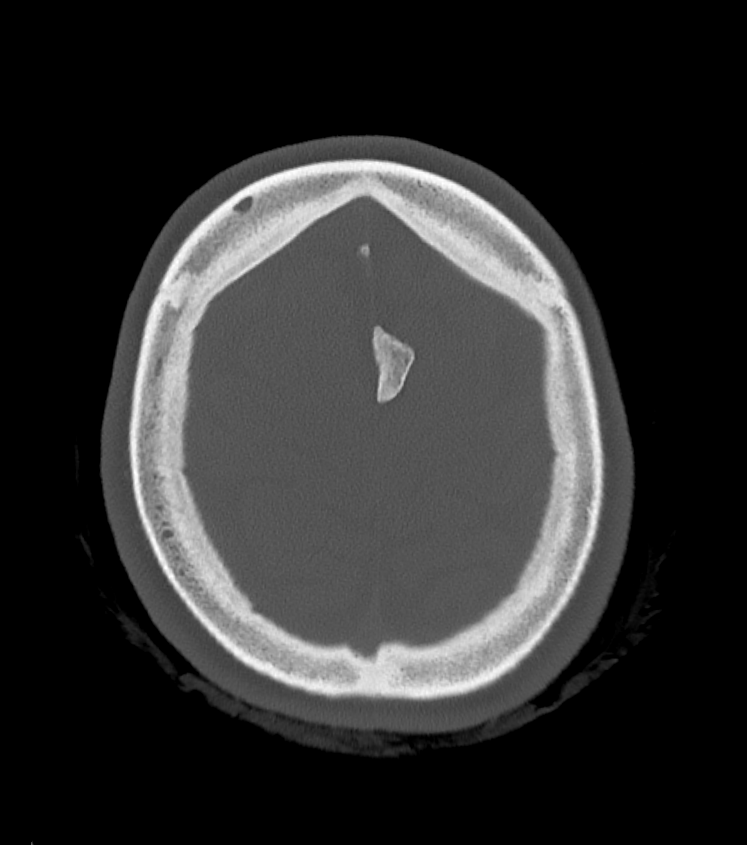
- Computed Tomography (CT):
- Linear or curvilinear hyperdense lesion along the falx cerebri
- May appear as single or multiple foci of calcification
- Hounsfield units similar to bone
- Magnetic Resonance Imaging (MRI):
- T1-weighted: Hypointense signal
- T2-weighted: Hypointense signal
- Susceptibility-weighted imaging (SWI): Marked hypointensity
- Plain radiographs:
- May be visible on lateral skull X-rays as linear calcification
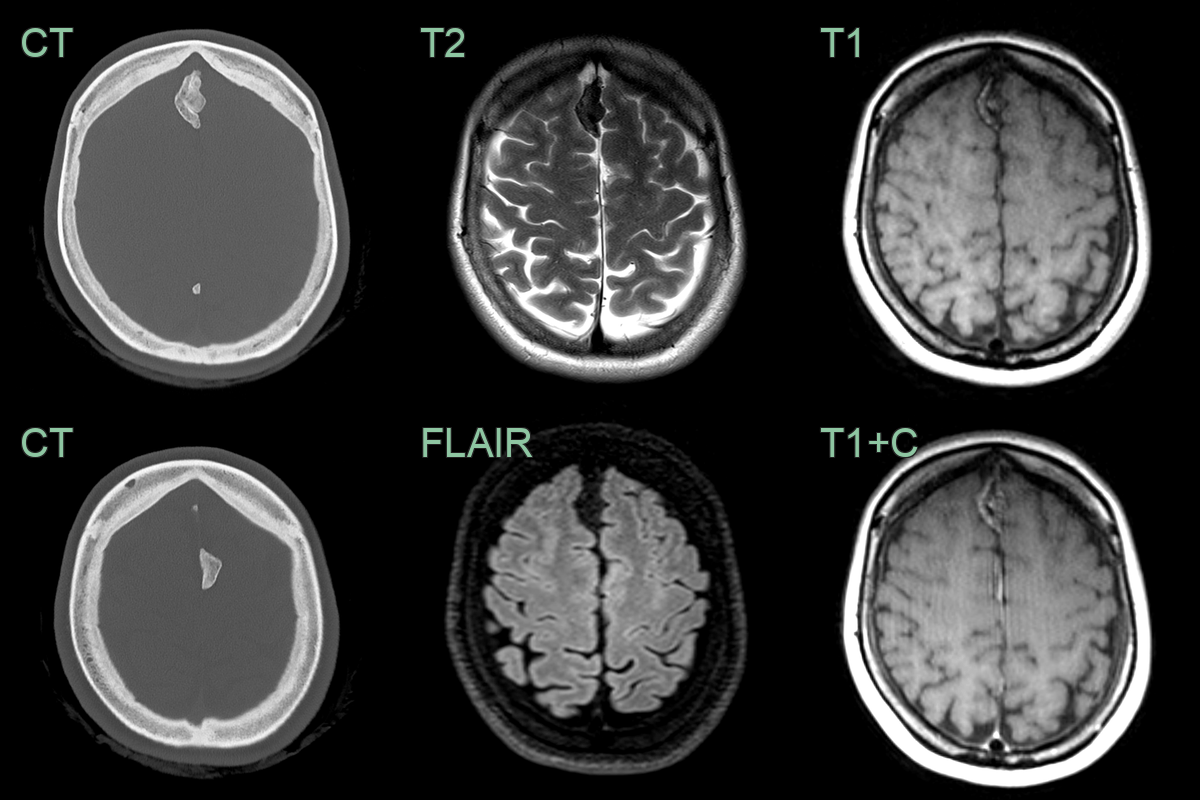
- A 50-year-old patient presented with headache.
- CT showed lobulated calcification of both sides of the falx.
- The T1-hyperintensity and lack of enhancement was consistent with ossification of the falx (rather than a meningioma).
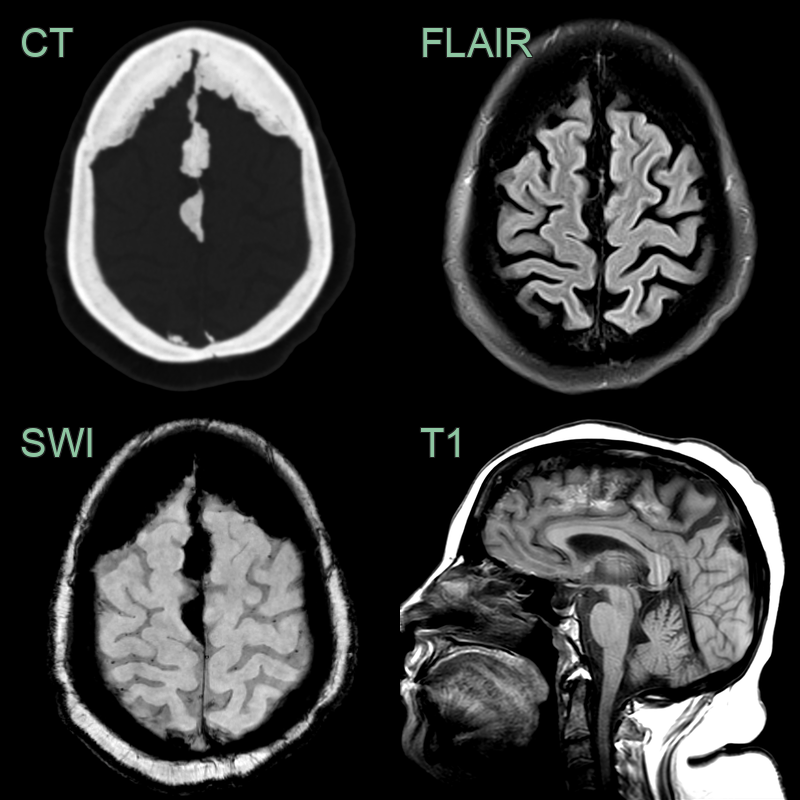
- Incidental finding of ossified falx cerebri with blooming on SWI and T1 shortening.
Treatment¶
- No specific treatment required for asymptomatic cases
- Management focuses on addressing any underlying metabolic disorders if present
- In rare symptomatic cases:
- Conservative management of headaches with analgesics
- Anticonvulsants for seizure control if necessary
- Surgical intervention generally not indicated unless complications arise
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Meningioma | Ossification of the falx cerebri is typically linear and thin, while meningiomas are more nodular or mass-like |
| Calcified subdural haematoma | Ossification of the falx is midline, while subdural haematomas are typically crescentic and follow the inner table of the skull |
| Dural metastases | Metastases often have irregular borders and multiple lesions, while falx ossification is smooth and singular |
| Psammomatous meningioma | Psammomatous meningiomas show punctate calcifications, while falx ossification is more continuous |
| Hyperostosis | Hyperostosis affects the skull bones, while falx ossification is within the intracranial space |
| Calcified epidural haematoma | Epidural haematomas are typically biconvex and do not cross suture lines, unlike falx ossification |
| Intracranial lipoma | Lipomas have fat density on CT, while falx ossification shows bone density |
| Sturge-Weber syndrome | Sturge-Weber calcifications are typically gyriform and cortical, not in the falx |
| Tuberous sclerosis | Tuberous sclerosis calcifications are often subependymal, not in the falx |
| Physiological calcification | Physiological calcifications are typically seen in the pineal gland or choroid plexus, not in the falx |