Ossification of the Posterior Longitudinal Ligament (OPLL)¶
Summary

- OPLL is a hyperostotic condition characterised by ectopic ossification of the posterior longitudinal ligament of the spine
- Most commonly affects the cervical spine, leading to spinal cord compression and myelopathy
- Diagnosis relies on clinical presentation and imaging findings, with CT and MRI being the modalities of choice
Pathophysiology¶
- Exact aetiology remains unclear, but involves:
- Genetic factors (e.g. COL6A1, BMP2, and TGF-β1 genes)
- Metabolic disorders (e.g. diabetes mellitus, obesity)
- Mechanical stress on the ligament
- Ossification process:
- Metaplasia of ligamentous cells to chondrocytes
- Subsequent endochondral ossification
- Progressive calcification and bone formation within the ligament
Demographics¶
- Prevalence:
- Higher in East Asian populations (2-4% in Japan)
- Less common in Western countries (0.1-1.7%)
- Age of onset:
- Typically presents in the 5th to 6th decade of life
- Gender distribution:
- Male predominance (2:1 to 3:1 male-to-female ratio)
Diagnosis¶
- Clinical presentation:
- Neck pain and stiffness
- Myelopathy symptoms (e.g. gait disturbance, hand clumsiness)
- Radiculopathy (less common)
- Physical examination:
- Decreased range of motion in the cervical spine
- Upper motor neuron signs (e.g. hyperreflexia, Hoffman's sign)
- Sensory deficits in the upper and lower extremities
- Classification:
- Continuous type
- Segmental type
- Mixed type
- Localised type (also known as circumscribed type)
Imaging¶
- Plain radiographs:
- Limited sensitivity, especially in early stages
- May show linear ossification along the posterior aspect of vertebral bodies
- Computed Tomography (CT):
- Gold standard for diagnosis and classification
- Demonstrates extent and morphology of ossification
- Helps in surgical planning
- Magnetic Resonance Imaging (MRI):
- Best for evaluating spinal cord compression and myelopathy
- T2-weighted images show hypointense signal of ossified ligament
- Useful for assessing disc herniations and other soft tissue abnormalities
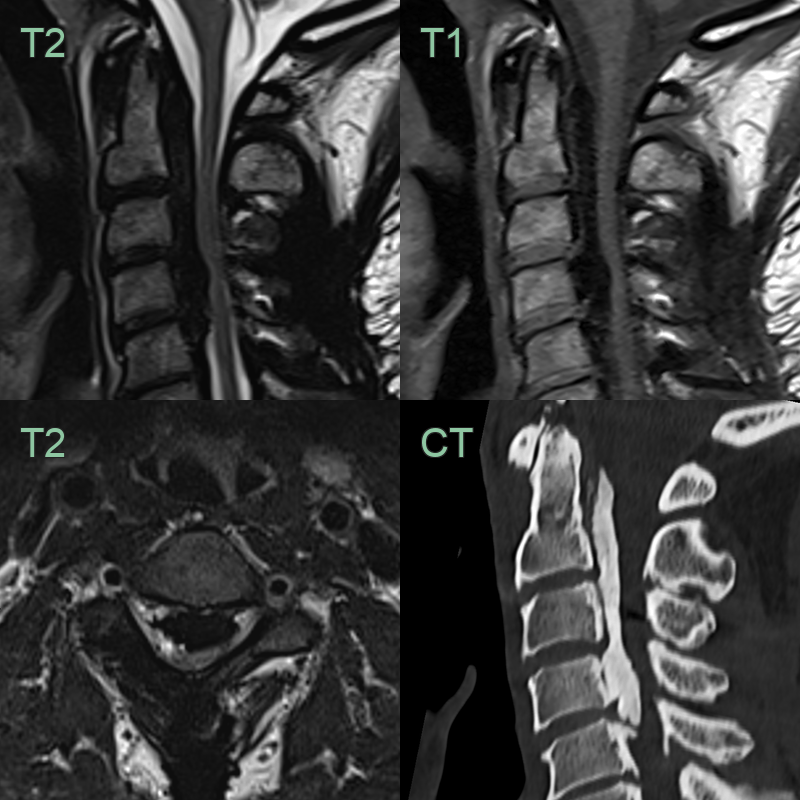
- 60-year-old patient with worsening myelopathy affecting the lower limbs.
- The vertebral canal stenosis was caused by a hypointense/hyperdense ossified posterior longitudinal ligament.
- The cord was compressed with mutliple short segments of myelopathic signal change.
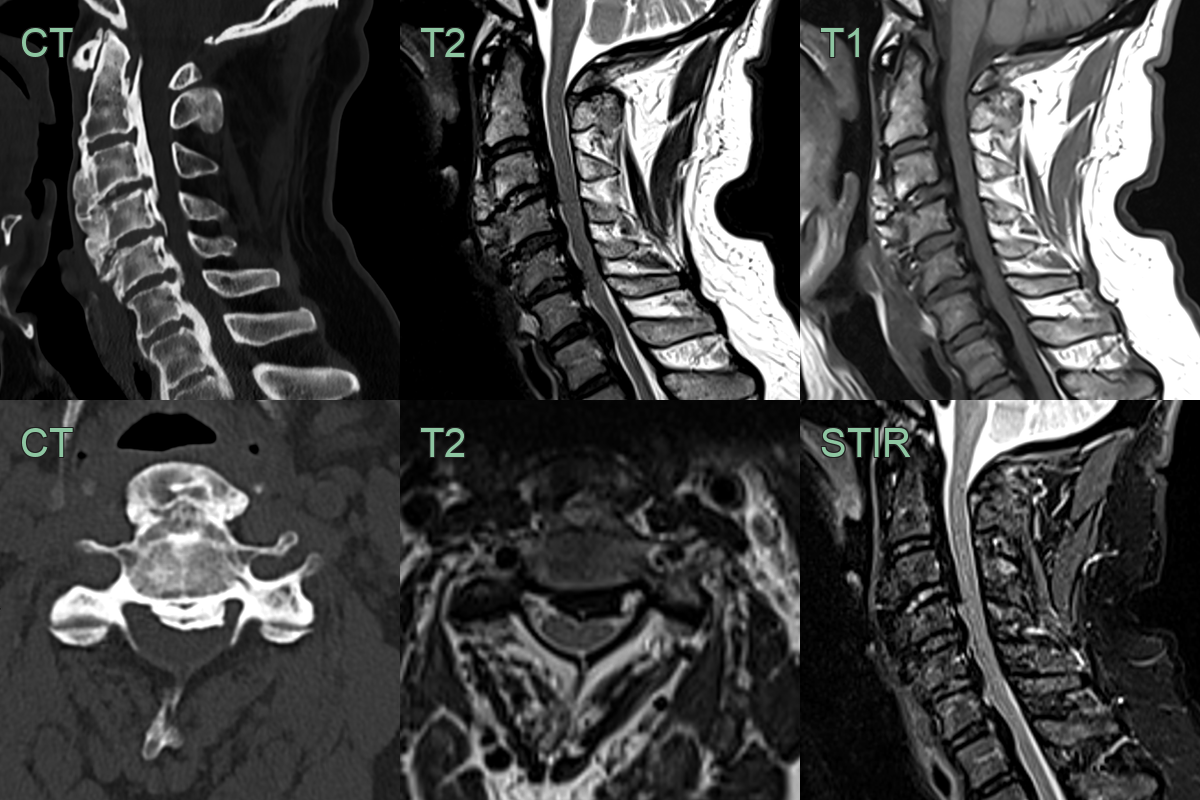
- A 70-year-old patient presented with a mild myelopathy affecting the lower limbs.
- CT showed extensive calcification and thickening of the posterior longitudinal ligament, which returned low signal on all MRI sequences.
- The cord was slightly flattened but there was no T2-hyperintense myelopathic signal change.
Treatment¶
- Conservative management:
- For mild cases or patients unfit for surgery
- Includes physical therapy, cervical collar, and pain management
- Surgical intervention:
- Indicated for progressive myelopathy or severe cord compression
- Anterior approach:
- Anterior cervical discectomy and fusion (ACDF)
- Anterior cervical corpectomy and fusion (ACCF)
- Posterior approach:
- Laminoplasty
- Laminectomy with or without fusion
- Combined anterior-posterior approach for severe cases
- Complications:
- Cerebrospinal fluid leakage
- C5 palsy
- Postoperative kyphosis
- Adjacent segment disease
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Diffuse Idiopathic Skeletal Hyperostosis (DISH) | Primarily affects anterior longitudinal ligament; OPLL affects posterior longitudinal ligament |
| Degenerative Disc Disease | Typically affects intervertebral discs; OPLL involves ossification of ligament |
| Cervical Spondylotic Myelopathy | Caused by degenerative changes; OPLL is a specific ossification process |
| Ankylosing Spondylitis | Primarily affects sacroiliac joints and spine; OPLL is localised to posterior longitudinal ligament |
| Spinal Cord Tumour | Presents as a focal mass; OPLL shows continuous or segmental ossification along the ligament |
| Herniated Cervical Disc | Acute onset, typically at a single level; OPLL is chronic and often multi-level |
| Rheumatoid Arthritis of the Cervical Spine | Affects facet joints and atlantoaxial articulation; OPLL affects the ligament |
| Fluorosis | Affects multiple bones and ligaments; OPLL is specific to posterior longitudinal ligament |
| Hypoparathyroidism | Causes generalized ligament calcification; OPLL is localised to posterior longitudinal ligament |
| Ossification of the Ligamentum Flavum | Affects ligamentum flavum; OPLL affects posterior longitudinal ligament |