Paraganglioma¶
Summary
- Rare neuroendocrine tumours arising from extra-adrenal paraganglia
- Typically present with symptoms related to catecholamine excess or mass effect
- Imaging plays crucial role in diagnosis, localization, and staging
Pathophysiology¶
- Derived from neural crest cells of the autonomic nervous system
- Can be functional (secreting catecholamines) or non-functional
- Associated with various genetic syndromes (e.g., SDHx mutations, VHL, NF1)
- Malignant potential in 10-20% of cases
Demographics¶
- Incidence: 2-8 per million person-years
- Peak incidence: 30-50 years old
- Slight male predominance
- Higher prevalence in patients with genetic predisposition syndromes
Diagnosis¶
- Clinical presentation:
- Hypertension (paroxysmal or sustained)
- Headaches, palpitations, sweating
- Abdominal pain or mass effect symptoms
- Biochemical testing:
- Plasma or urinary metanephrines and catecholamines
- Chromogranin A levels
- Genetic testing for associated syndromes
Imaging¶
- CT:
- Contrast-enhanced CT: hypervascular, well-defined masses
- Washout characteristics differ from adrenal adenomas
- MRI:
- T1: iso- to hypointense
- T2: markedly hyperintense ("light bulb" sign)
- Strong enhancement on post-contrast images
- Functional imaging:
- 123I-MIBG scintigraphy: high specificity for paragangliomas
- 68Ga-DOTATATE PET/CT: superior sensitivity, especially for SDHx-related tumours
- 18F-FDG PET/CT: useful for detecting metastatic disease
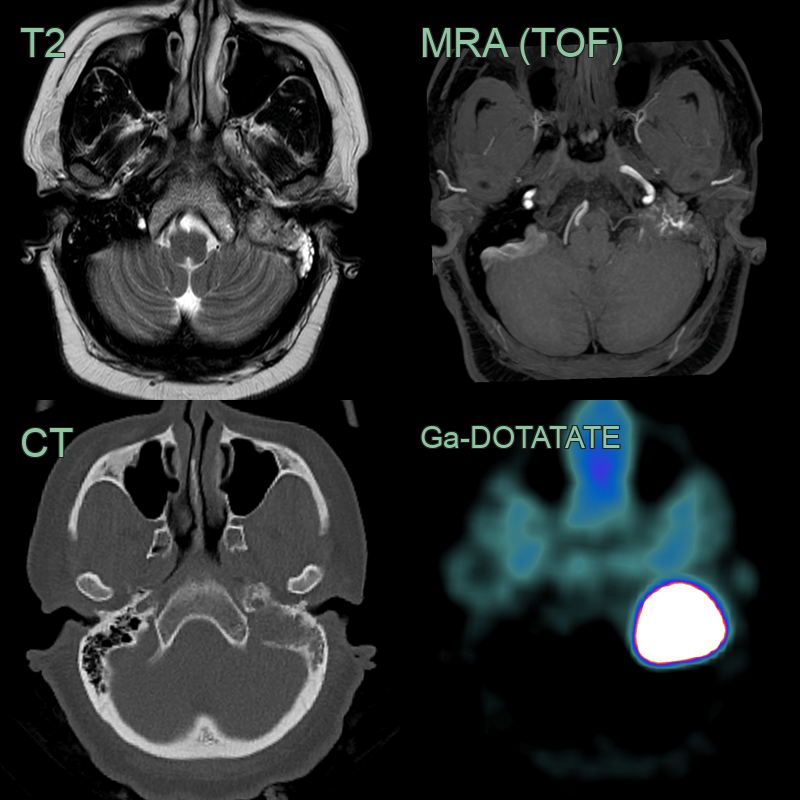
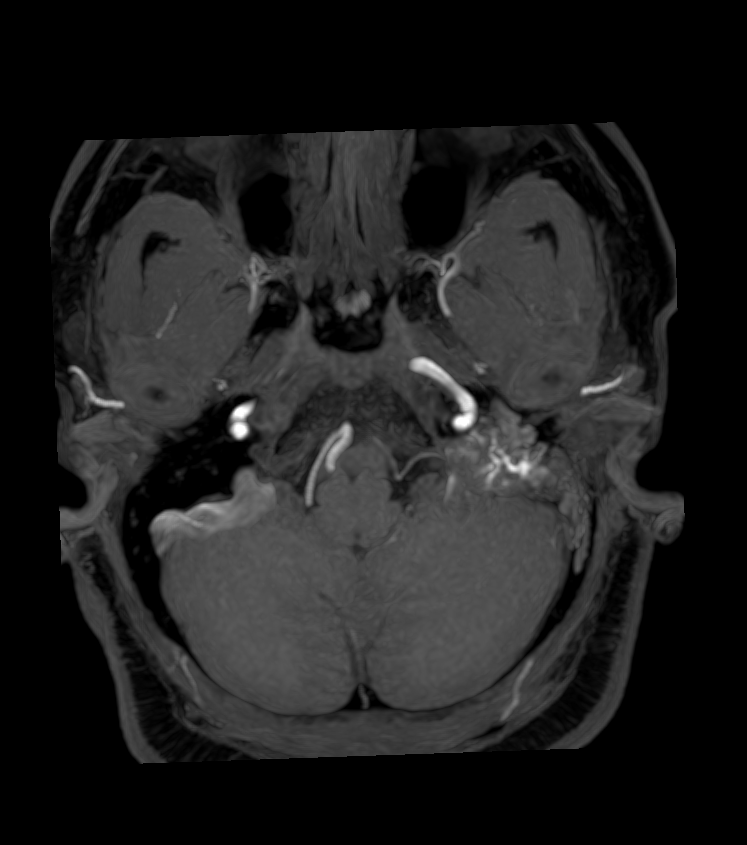
- 40-year-old patient presented with hearing loss and facial palsy.
- MRI showed a lesion in the left jugular foramen and petromastoid bone with evidence of vascularity on T2-weighted imaging (i.e., flow voids) and time-of-flight angiography. Ga-DOTATATE PET showed avid tracer uptake as expected in a paraganglioma.
Treatment¶
- Surgical resection: primary treatment modality
- Preoperative management:
- Alpha-adrenergic blockade (e.g., phenoxybenzamine)
- Beta-blockers as adjunct therapy
- Radiotherapy: for unresectable or metastatic disease
- Systemic therapies:
- 131I-MIBG therapy for MIBG-avid tumours
- Peptide receptor radionuclide therapy (PRRT) for somatostatin receptor-positive tumours
- Chemotherapy for rapidly progressive disease
- Long-term follow-up: essential due to risk of recurrence and metastasis
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Pheochromocytoma | Located in adrenal gland, while paragangliomas are extra-adrenal |
| Carotid body tumour | Specifically located at carotid bifurcation, "lyre sign" on angiography |
| Schwannoma | Typically encapsulated, heterogeneous enhancement on MRI |
| Metastatic lymph node | Irregular borders, loss of fatty hilum on imaging |
| Glomus tympanicum | Located in middle ear, associated with pulsatile tinnitus |
| Meningioma | Dural tail sign on MRI, calcifications more common |
| Vagal paraganglioma | Splays carotid bifurcation anteriorly (unlike carotid body tumour) |
| Aneurysm | Pulsatile, shows flow on Doppler ultrasound |
| Neurofibroma | Associated with café-au-lait spots, target sign on MRI |