Posterior Cerebral Artery (PCA) infarct
Summary
- Ischaemic stroke affecting the territory supplied by the posterior cerebral artery
- Presents with visual field defects, sensory deficits, and cognitive impairment
- Diagnosis confirmed by neuroimaging, typically CT or MRI
Pathophysiology
- Occlusion of the PCA or its branches, leading to ischaemia in the supplied territory
- Common causes:
- Embolism (cardiac or arterial)
- Atherosclerosis
- Dissection
- Vasculitis
- Affected areas may include:
- Occipital lobe
- Medial temporal lobe
- Thalamus
- Midbrain
Demographics
- Accounts for approximately 5-10% of all ischaemic strokes
- Risk factors:
- Hypertension
- Diabetes mellitus
- Atrial fibrillation
- Smoking
- Hyperlipidaemia
- More common in older adults, but can occur at any age
Diagnosis
- Clinical presentation:
- Homonymous hemianopia or quadrantanopia
- Cortical blindness (bilateral PCA infarcts)
- Sensory deficits
- Memory impairment
- Visual agnosia
- Prosopagnosia
- Neurological examination
- Neuroimaging (CT or MRI)
- Vascular imaging (CT angiography, MR angiography, or conventional angiography)
Imaging
- Non-contrast CT:
- Early: may be normal or show subtle hypodensity in PCA territory
- Late: well-defined hypodense area in PCA territory
- CT angiography:
- May demonstrate occlusion or stenosis of PCA
- MRI:
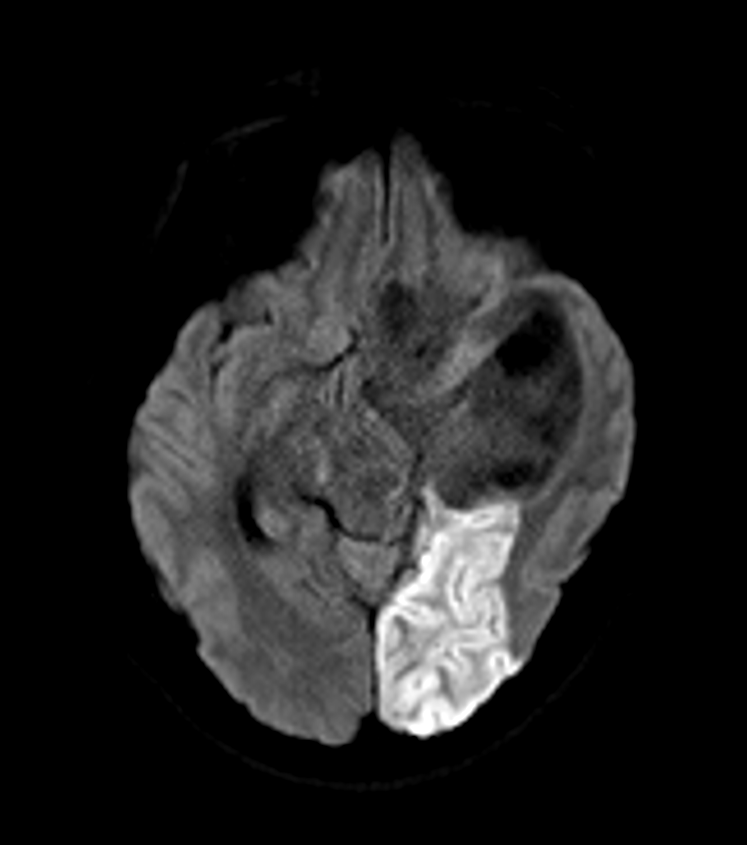
- Diffusion-weighted imaging (DWI): early detection of acute infarction
- T2-weighted and FLAIR: hyperintense signal in affected areas
- Susceptibility-weighted imaging (SWI): may show thrombus as blooming artefact
- MR angiography:
- Visualisation of PCA occlusion or stenosis
- Perfusion imaging (CT or MRI):
- May demonstrate perfusion-diffusion mismatch in acute setting
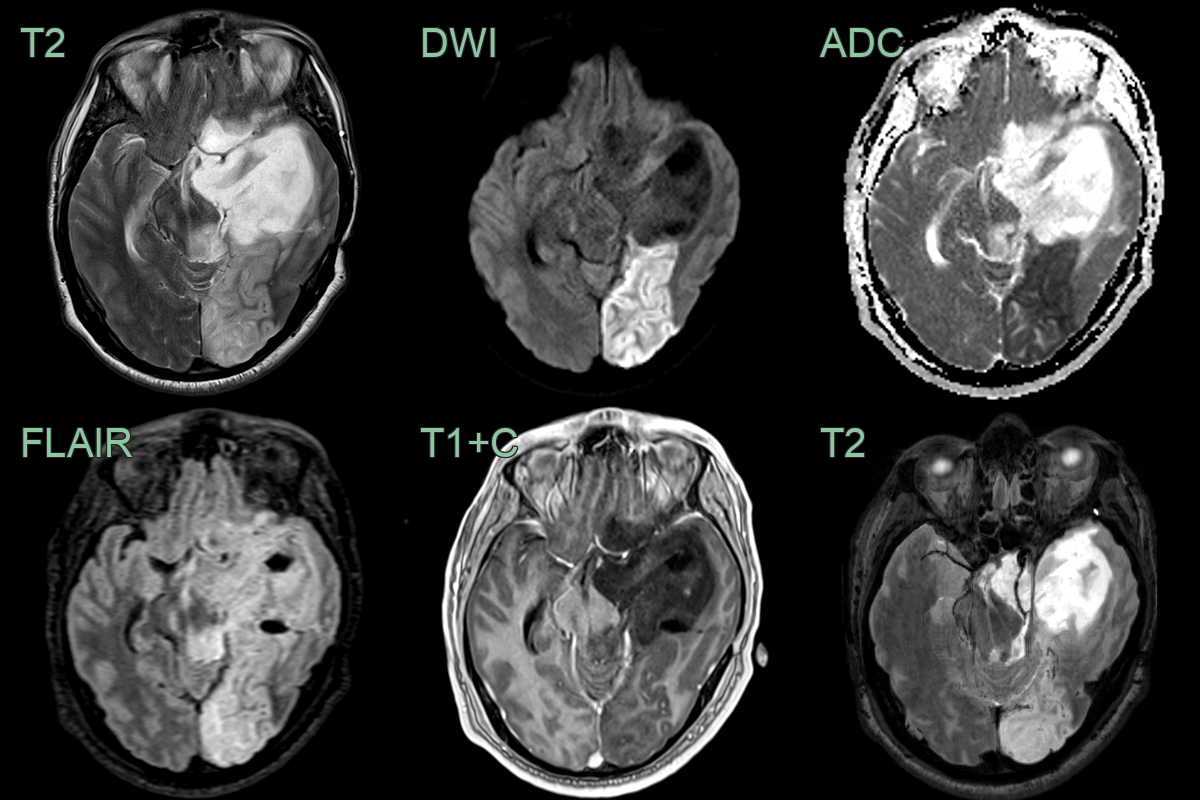
- 30-year-old patient with a grade 2 astrocytoma presented with a right visual field defect.
- MRI showed an acute infarct presumably due to occlusion of the left PCA that was encased in tumour.
Treatment
- Acute management:
- Intravenous thrombolysis within 4.5 hours of symptom onset
- Mechanical thrombectomy in selected cases (proximal PCA occlusion)
- Secondary prevention:
- Antiplatelet therapy
- Anticoagulation if cardioembolic source
- Risk factor modification (blood pressure control, diabetes management, smoking cessation)
- Rehabilitation:
- Visual rehabilitation for hemianopia
- Occupational therapy for cognitive deficits
- Speech and language therapy if needed
- Long-term follow-up and monitoring for recurrence
Differential diagnosis
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Middle Cerebral Artery (MCA) infarct | Spares occipital lobe and medial temporal lobe |
| Migraine with aura | Symptoms are typically transient and resolve within an hour |
| Occipital lobe tumour | Gradual onset of symptoms and presence of mass effect on imaging |
| Herpes simplex encephalitis | Fever, altered mental status, and bilateral temporal lobe involvement |
| Posterior Reversible Encephalopathy Syndrome (PRES) | Reversible vasogenic oedema, often bilateral and symmetrical |
| Carbon monoxide poisoning | Bilateral globus pallidus involvement on imaging |
| Basilar artery thrombosis | Brainstem symptoms and "top of the basilar" syndrome |
| Venous sinus thrombosis | Presence of haemorrhage and venous congestion on imaging |
| Mitochondrial encephalopathy (MELAS) | Stroke-like lesions not confined to vascular territories |
| Hypoglycemia | Global reduction in brain metabolism, reversible with glucose administration |