Perineural Spread of Tumour¶
Summary

- Perineural spread (PNS) involves tumour cells invading and spreading along nerve sheaths
- Commonly seen in head and neck cancers, particularly squamous cell carcinoma
- Imaging plays a crucial role in detection and staging, with MRI being the modality of choice
Pathophysiology¶
- Tumour cells infiltrate nerve sheaths, typically along the path of least resistance
- Spread occurs bidirectionally along nerves, both proximally and distally
- Mechanisms involve:
- Direct invasion of nerves by tumour cells
- Lymphatic spread within nerve sheaths
- Haeatogenous spread to nerves
Demographics¶
- Most common in head and neck cancers:
- Squamous cell carcinoma (50-80% of cases)
- Adenoid cystic carcinoma
- Mucoepidermoid carcinoma
- Other tumours with PNS include:
- Melanoma
- Lymphoma
- Prostate cancer
- Incidence increases with:
- Advanced tumour stage
- Poor differentiation
- Larger tumour size
Diagnosis¶
- Clinical presentation:
- Often asymptomatic in early stages
- Neurological symptoms (e.g., pain, numbness, weakness) when advanced
- Histopathological examination:
- Gold standard for definitive diagnosis
- Challenging due to skip lesions and discontinuous spread
- Imaging:
- Essential for early detection and accurate staging
Imaging¶
- MRI:
- Modality of choice for detecting PNS
- High-resolution T1-weighted sequences with fat suppression
- Gadolinium enhancement improves detection
- Key findings:
- Nerve enlargement and enhancement
- Loss of perineural fat plane
- Muscular denervation changes
- CT:
- Useful for bony involvement and skull base erosion
- Less sensitive than MRI for soft tissue involvement
- PET/CT:
- Helpful in detecting distant metastases
- Limited sensitivity for early PNS
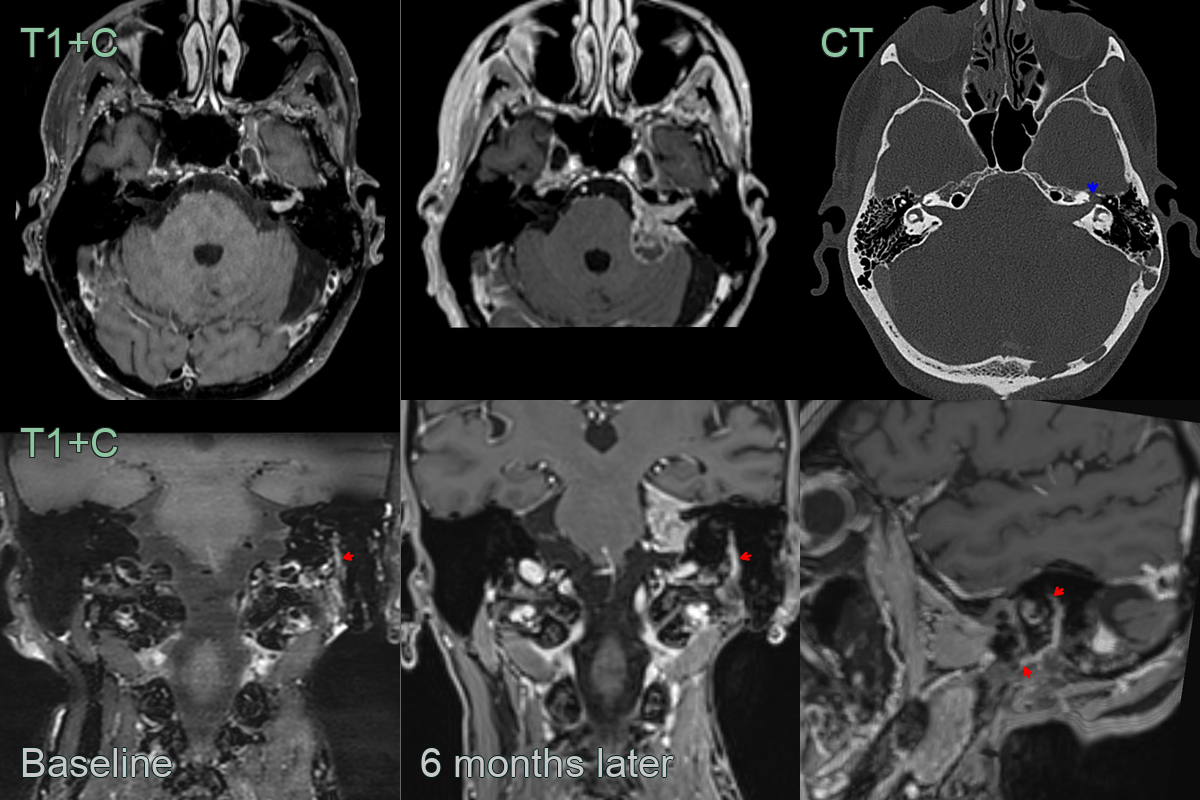
- A 70-year-old patient underwent an MRI as part of surveillance for following radical parotidectomy and radiotherapy.
- On the first scan, there was pathological enhancement filling the left internal auditory canal and along the length on the facial nerve down to its mastoid section (red arrows).
- 6 months later, the intracranial component of the tumour has enlarged and there was extension of the facial nerve thickening and enhancement.
- The CT showed remodelling of bone around the facial geniculate ganglion (blue arrow).
Treatment¶
- Multidisciplinary approach:
- Surgery
- Radiotherapy
- Chemotherapy
- Surgical management:
- Wide local excision with clear margins
- Nerve sacrifice may be necessary in extensive PNS
- Radiotherapy:
- Often used as adjuvant treatment
- Extended fields to cover potential areas of spread
- Chemotherapy:
- Role in advanced or recurrent disease
- Often combined with radiotherapy
- Prognosis:
- Presence of PNS associated with poorer outcomes
- Early detection and appropriate treatment crucial for improved survival
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Bell's palsy | Enhancement of facial nerve without discrete perineural thickening; no skull base foramen enlargement |
| Schwannoma | Well-defined, encapsulated enhancing mass along a single nerve; does not involve multiple branches |
| Neurofibroma | Fusiform nerve expansion; may involve multiple nerves in NF1; "target sign" on T2-weighted MRI |
| Lymphoma | Diffuse nerve infiltration; associated cervical lymphadenopathy; lacks discrete skip lesions |
| Sarcoidosis | Cranial nerve enhancement with associated leptomeningeal enhancement; hilar lymphadenopathy on chest imaging |
| Leptomeningeal carcinomatosis | Diffuse leptomeningeal enhancement; multiple cranial nerve involvement simultaneously; hydrocephalus |