Petrous Cephalocele¶
Summary
- Rare congenital or acquired herniation of intracranial contents through a defect in the petrous temporal bone
- Typically presents with cerebrospinal fluid (CSF) otorrhea or recurrent meningitis
- Imaging shows a defect in the petrous bone with herniation of brain tissue and/or meninges
Pathophysiology¶
- Congenital:
- Result of incomplete ossification of the petrous temporal bone during development
- Associated with other temporal bone anomalies
- Acquired:
- Secondary to trauma, surgery, or erosive processes (e.g., cholesteatoma)
- Increased intracranial pressure may contribute to herniation
Demographics¶
- Rare condition, exact prevalence unknown
- Congenital cases:
- Usually diagnosed in childhood or early adulthood
- No significant gender predilection
- Acquired cases:
- Can occur at any age
- More common in adults with a history of trauma or surgery
Diagnosis¶
- Clinical presentation:
- CSF otorrhea
- Recurrent meningitis
- Hearing loss
- Headache
- Physical examination:
- Otoscopy may reveal fluid in the middle ear
- Positive "reservoir sign" (fluid accumulation in external auditory canal when compressed)
- Laboratory tests:
- Beta-2 transferrin assay of ear fluid to confirm CSF
Imaging¶
- High-resolution CT (HRCT) of the temporal bone:
- Defect in the petrous temporal bone
- Bony dehiscence of the tegmen tympani or mastoid
- Air-fluid level in the middle ear or mastoid
- MRI:
- T2-weighted sequences show herniation of brain tissue and/or meninges
- CISS/FIESTA sequences helpful for detecting small defects
- Potential complications (e.g., meningocele, encephalocele)
- CT cisternography:
- Contrast medium in the subarachnoid space to identify CSF fistula
- Useful when the defect is not clearly visible on HRCT or MRI
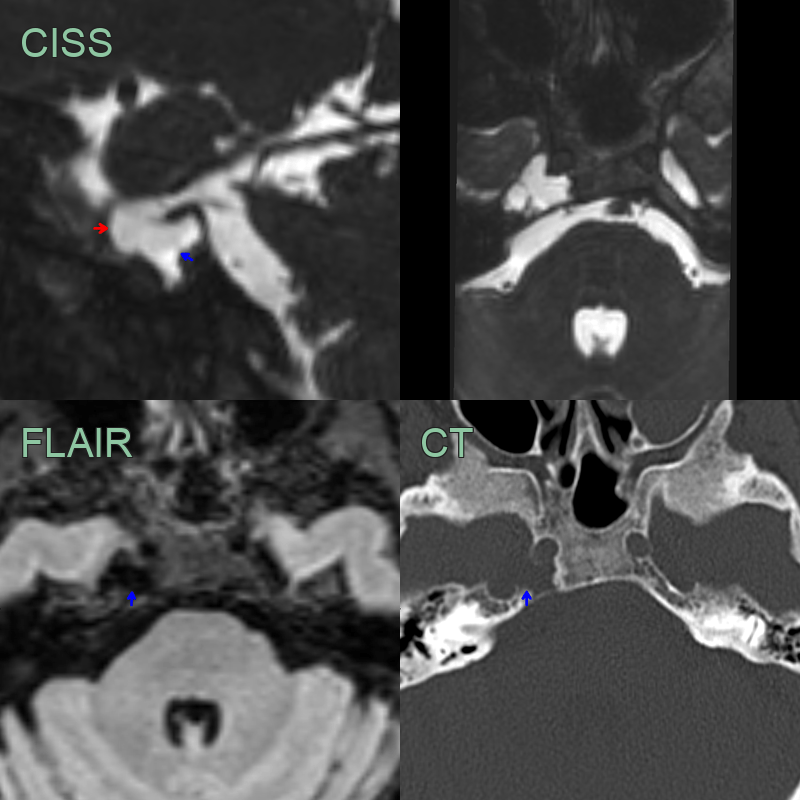
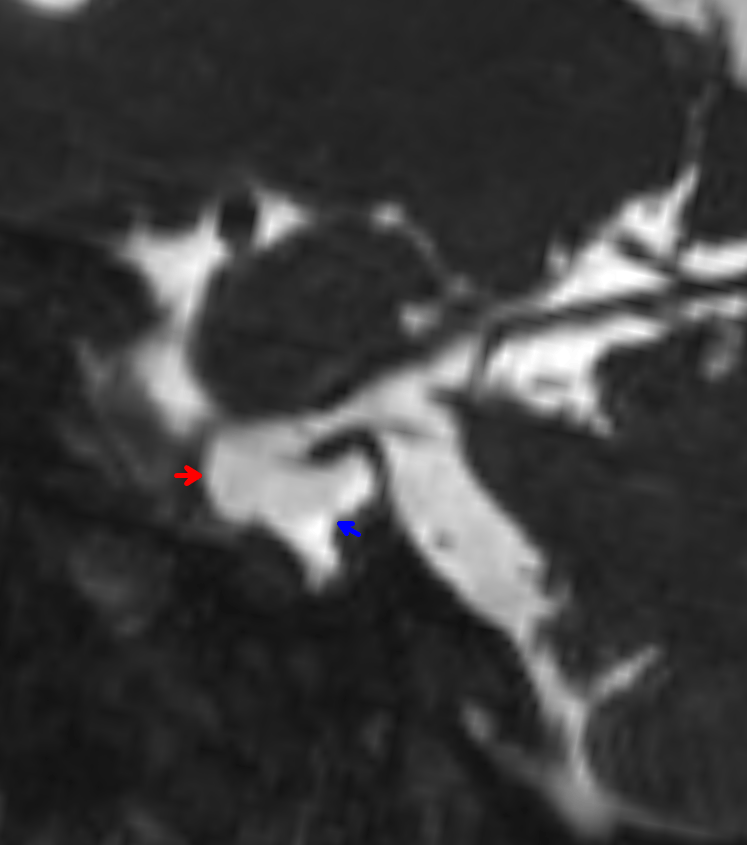
- Incidental finding of a CSF filled structure in the petrous apex (blue arrow).
- The cephalocele was contiguous with Meckel's cave (red arrow).
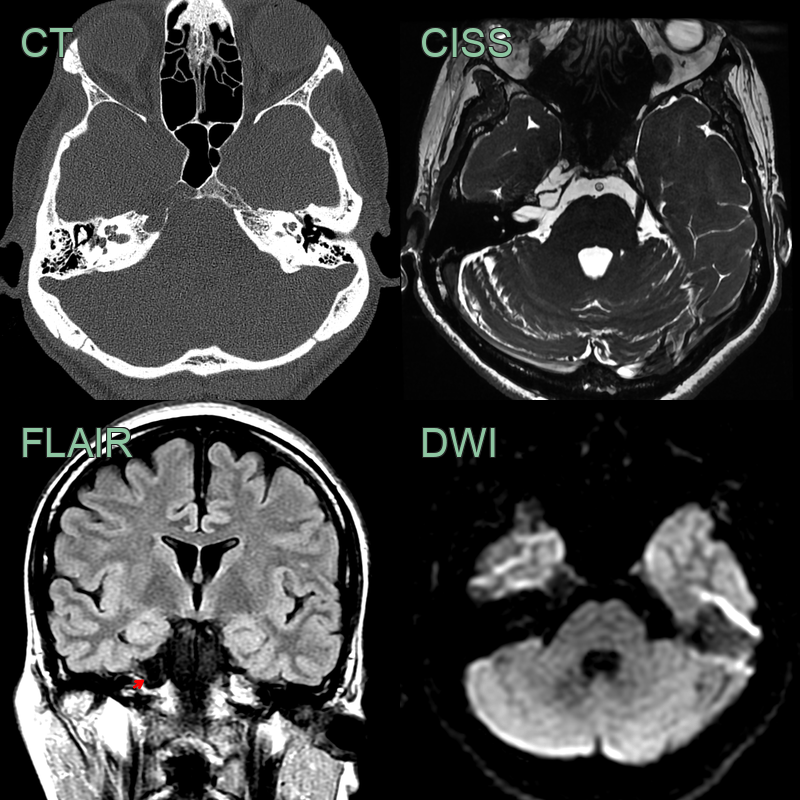
- A 50-year-old patient presentd with right sided trigeminal neuralgia.
- CT showed a well demarcated excavation of the right petrous apex.
- The cavity was filled with CSF with no enhancement of diffusion restriction.
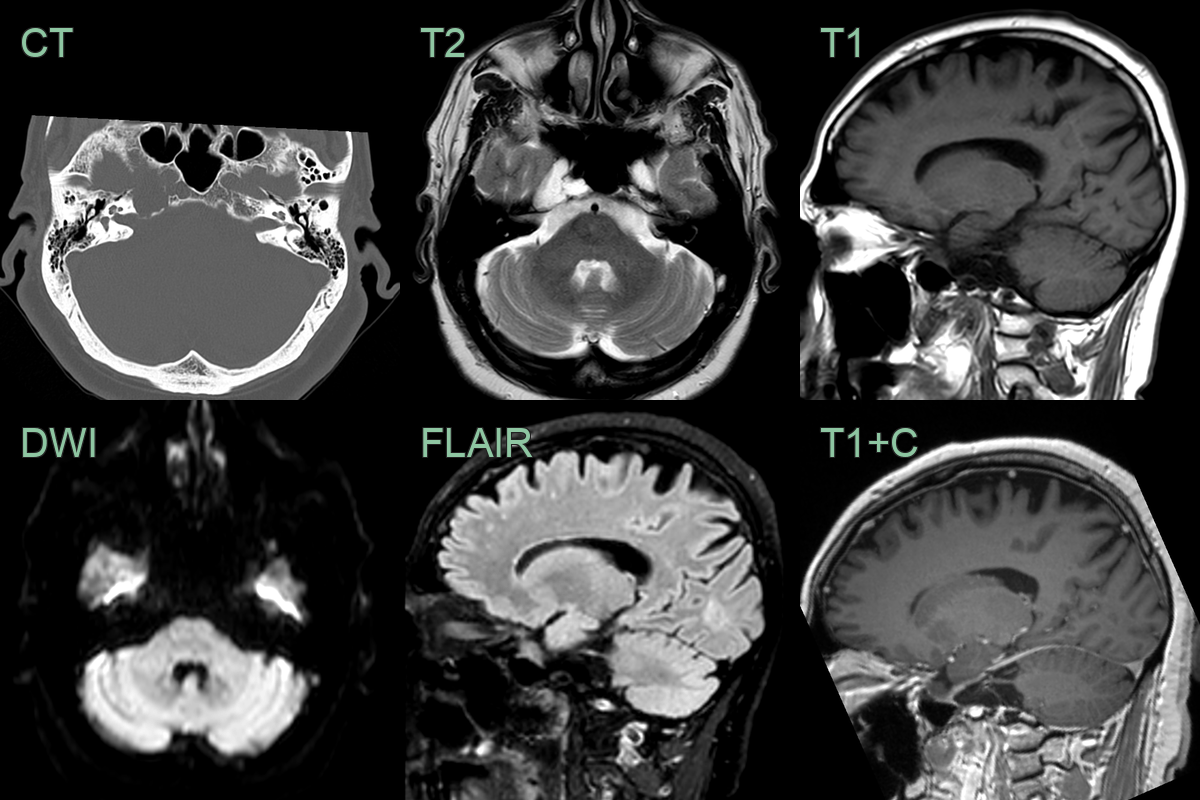
- A 60-year-old patient presented with headache.
- CT showed a well-marginated lesion remodelling the right petrous apex.
- MRI did not show any abnormal soft tissue or enhancement with only CSF signal content.
Treatment¶
- Conservative management:
- Bed rest with head elevation
- Avoidance of activities that increase intracranial pressure
- Surgical repair:
- Transmastoid approach
- Middle cranial fossa approach
- Combined approach for larger defects
- Surgical techniques:
- Autologous materials (fascia, cartilage, bone)
- Synthetic materials (hydroxyapatite cement)
- Multilayer closure for improved success rates
- Post-operative care:
- CSF diversion (lumbar drain) to reduce pressure on repair site
- Antibiotic prophylaxis to prevent meningitis
- Follow-up imaging:
- HRCT or MRI to confirm successful repair and monitor for recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Cholesterol Granuloma | Lacks communication with subarachnoid space; hyperintense on T1-weighted MRI |
| Arachnoid Cyst | Follows CSF signal on all MRI sequences; no enhancement |
| Epidermoid Cyst | Restricted diffusion on DWI; may have calcifications |
| Petrous Apex Mucocele | No communication with subarachnoid space; may show peripheral enhancement |
| Meningioma | Homogeneous enhancement; dural tail sign |
| Schwannoma | Enhancing mass centered on internal auditory canal |
| Chordoma | Destructive midline lesion; T2 hyperintense with heterogeneous enhancement |
| Petrous Apex Effusion | No mass effect; fluid signal without enhancement |
| Aneurysm | Flow voids on MRI; intense enhancement on CTA/MRA |
| Paraganglioma | Salt-and-pepper appearance on T2; intense enhancement |