Pineal Tumour of Intermediate Differentiation¶
Summary
- Rare neoplasm of the pineal gland with mixed features of pineocytoma and pineoblastoma
- Clinical presentation includes headache, visual disturbances, and Parinaud syndrome
- Imaging shows a well-defined, heterogeneous mass in the pineal region with variable enhancement
Pathophysiology¶
- Arises from pineal parenchymal cells
- WHO grade 2 or 3 tumour, depending on mitotic activity and neurofilament protein expression
- Exhibits intermediate differentiation between pineocytoma and pineoblastoma
- May show areas of necrosis and calcification
Demographics¶
- Rare tumour, accounting for <0.1% of all intracranial neoplasms
- Typically affects young adults and middle-aged individuals
- No significant gender predilection reported
Diagnosis¶
- Clinical presentation:
- Headache
- Visual disturbances
- Parinaud syndrome (vertical gaze palsy, convergence-retraction nystagmus)
- Hydrocephalus due to compression of the cerebral aqueduct
- Histopathology:
- Moderate cellularity with diffuse growth pattern
- Intermediate nuclear-to-cytoplasmic ratio
- Mild to moderate nuclear atypia
- Immunohistochemistry positive for synaptophysin and neurofilament protein
Imaging¶
- CT:
- Well-defined, hyperdense mass in the pineal region
- Variable calcification patterns
- Contrast enhancement may be heterogeneous
- MRI:
- T1: Iso- to hypointense
- T2: Iso- to hyperintense
- T1 post-contrast: Heterogeneous enhancement
- DWI: Variable restricted diffusion
- MR spectroscopy: Elevated choline peak, reduced N-acetylaspartate
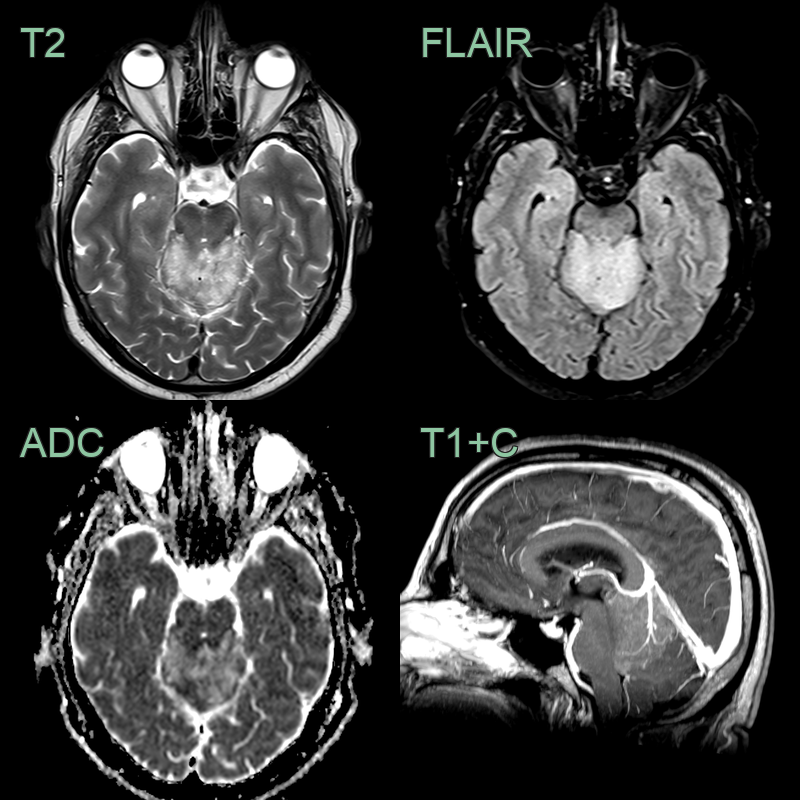
- A 50-year-old patient presented with a 6 month history of occipital headaches.
- MRI showed a lesion in the pineal region. A large vein within the lesion indicated that the lesion was extra-axial.
- Following resection, a pineal tumour of intermediate differentation (grade 3) was diagnosed.
Treatment¶
- Surgical resection:
- Gross total resection is the primary goal
- Endoscopic biopsy may be performed for initial diagnosis
- Adjuvant radiotherapy:
- Recommended for residual tumour or high-grade histology
- Craniospinal irradiation may be considered for disseminated disease
- Chemotherapy:
- Role is not well-established
- May be used in combination with radiotherapy for high-grade tumours or recurrent disease
- Regular follow-up imaging:
- MRI at 3-month intervals for the first year, then every 6-12 months
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Pineoblastoma | More cellular and less differentiated; higher mitotic activity; WHO grade 4 |
| Pineocytoma | Less cellular and well differentiated; minimal mitotic activity; WHO grade 1 |
| Germinoma | Absence of syncytiotrophoblastic giant cells and typical germ cell markers |
| Ependymoma | Lack of true ependymal rosettes and perivascular pseudorosettes |
| Astrocytoma | Absence of GFAP-positive neoplastic astrocytes |
| Meningioma | Lack of whorling pattern and psammoma bodies |
| Metastasis | Absence of history of primary cancer and different immunohistochemical profile |
| Pineal cyst | Solid components and enhancement on imaging, not purely cystic |
| Choroid plexus papilloma | Lack of papillary architecture and choroid plexus differentiation |
| Oligodendroglioma | Absence of characteristic "fried egg" appearance and 1p/19q codeletion |