Pituitary Apoplexy¶
Summary
- Acute clinical syndrome due to sudden haemorrhage or infarction of the pituitary gland
- Often occurs in patients with pre-existing pituitary adenomas
- Characterised by sudden onset of headache, visual disturbances, and hormonal dysfunction
Pathophysiology¶
- Rapid expansion of pituitary gland due to:
- Haemorrhage within a pituitary tumour
- Infarction of pituitary tissue
- Leads to:
- Compression of surrounding structures
- Potential ischaemia of normal pituitary tissue
- Risk factors:
- Anticoagulation therapy
- Major surgery
- Pregnancy
- Head trauma
- Hypertension
Demographics¶
- Incidence: 0.6-9.1% of all pituitary tumours
- Mean age at presentation: 50-60 years
- Male to female ratio: 1.5:1
- Most common in patients with macroadenomas (>10mm)
Diagnosis¶
- Clinical presentation:
- Sudden severe headache (95%)
- Visual disturbances (62%)
- Decreased visual acuity
- Visual field defects
- Ocular palsies (40%)
- Nausea and vomiting (69%)
- Altered mental status (19%)
- Laboratory findings:
- Hypopituitarism (80%)
- Hyponatremia
- Mild hyperprolactinemia
Imaging¶
- CT:
- Acute phase: Hyperdense lesion within pituitary fossa
- Subacute phase: Mixed density lesion
- Limited sensitivity (21-28%)
- MRI (preferred modality):
- T1-weighted:
- Acute: Isointense to hyperintense
- Subacute: Hyperintense due to methaemoglobin
- T2-weighted:
- Variable signal intensity
- Contrast-enhanced:
- Rim enhancement of the lesion
- Fluid-fluid levels may be present
- Sensitivity: 88-90%
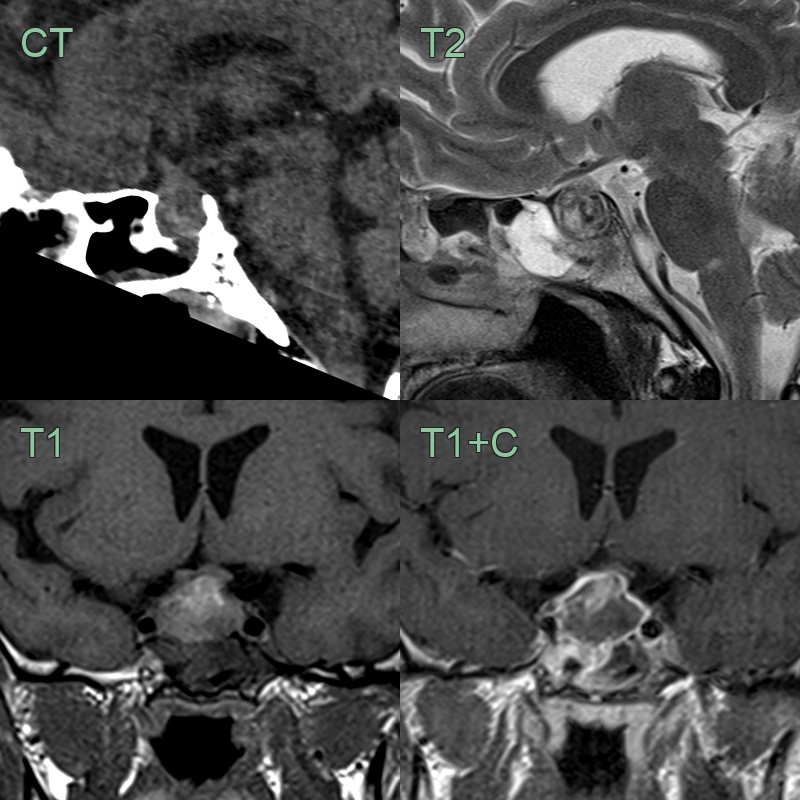
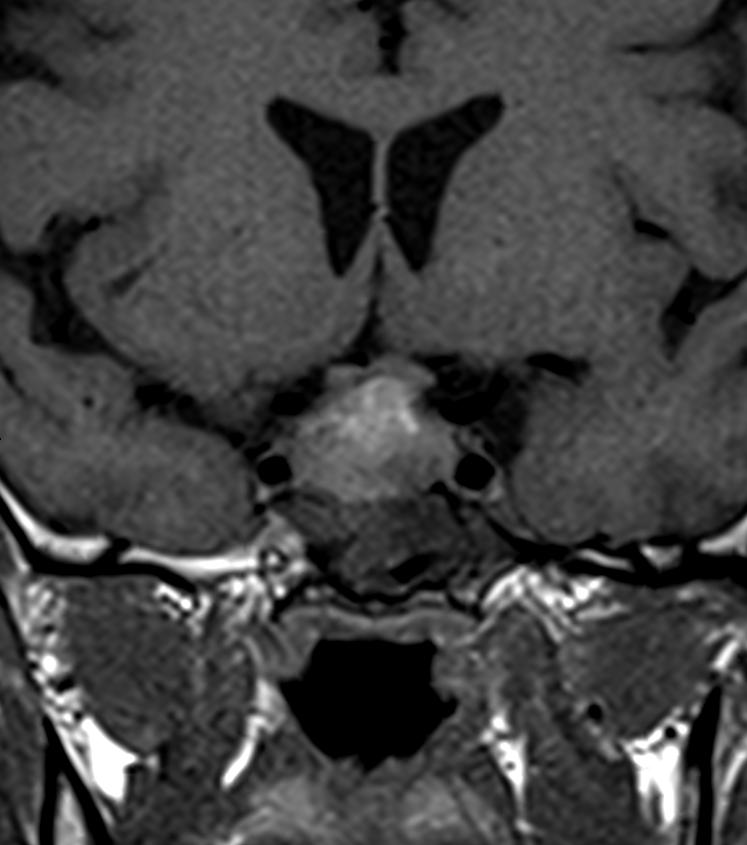
- 45-year-old patient presented with sudden onset headache and vomitting.
- CT showed subtle hyperdensity within an enlarged pituitary gland and dehisence of the floor of the fossa.
- MRI showed a heterogenously enlarged pituitary gland with T1-shortening, consistent with haemorrhage.
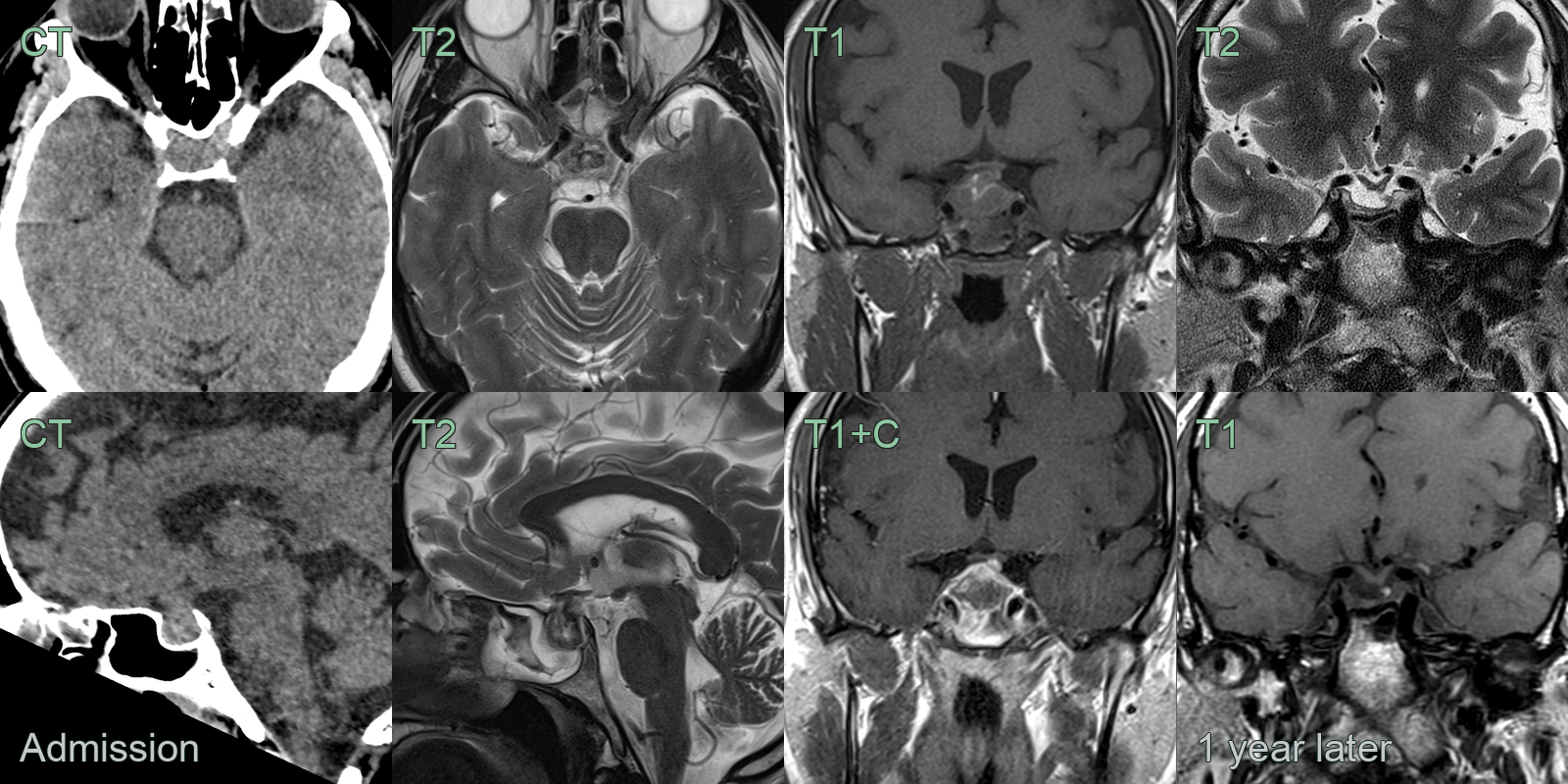
- A 40-year-old patient presented with sudden onset headache and vomitting.
- CT showed an increased soft tissue within the pituitary fossa with hyperdense acute blood product.
- MRI showed T1-hyperintense and T2-hypointense blood product with peripheral enhancement of normal pituitary tissue.
- There was contact, without compression, of the optic chiasm.
- One year later, without surgery, the volume of soft tissue within the fossa significantly decreased.
Treatment¶
- Initial management:
- Haemodynamic stabilization
- Corticosteroid replacement
- Correction of electrolyte imbalances
- Surgical intervention:
- Transsphenoidal surgery for:
- Severe visual impairment
- Altered mental status
- Progressive neurological deterioration
- Conservative management:
- For patients with mild symptoms and stable condition
- Close monitoring and hormonal replacement therapy
- Long-term follow-up:
- Regular endocrine evaluation
- Imaging surveillance
- Hormone replacement as needed
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Aneurysm (thrombosed parasellar) | Layered haemorrhage with peripheral flow void; arterial origin on MRA/CTA |
| Rathke cleft cyst haemorrhage | Non-enhancing T1 hyperintense sellar collection without solid component |
| Craniopharyngioma (haemorrhagic) | Suprasellar cystic/solid mass with calcifications on CT |
| Pituitary macroadenoma (non-haemorrhagic) | Enhancing sellar mass without blood products on T1/GRE |