Pituitary Macroadenoma¶
Summary
- Benign tumour of the pituitary gland >10mm in size
- Presents with mass effect symptoms and/or hormonal dysfunction
- Characterised by sellar expansion and suprasellar extension on imaging
Pathophysiology¶
- Arise from adenohypophyseal cells of the anterior pituitary
- Can be functional (hormone-secreting) or non-functional
- Growth leads to compression of surrounding structures:
- Optic chiasm
- Cavernous sinus
- Hypothalamus
- Hormonal imbalances due to:
- Excessive hormone production (in functional adenomas)
- Pituitary gland compression (hypopituitarism)
Demographics¶
- Peak incidence: 30-60 years of age
- Slight female predominance (1.2:1)
- Accounts for 10-15% of intracranial neoplasms
- Prevalence: 1 in 1000 in the general population
Diagnosis¶
- Clinical presentation:
- Mass effect symptoms:
- Headache
- Visual field defects (classically bitemporal hemianopsia)
- Cranial nerve palsies
- Hormonal symptoms (depending on tumour functionality):
- Prolactinoma: Galactorrhea, amenorrhea, infertility
- Growth hormone-secreting: Acromegaly or gigantism
- ACTH-secreting: Cushing's disease
- TSH-secreting: Hyperthyroidism
- Laboratory tests:
- Serum hormone levels (prolactin, GH, IGF-1, ACTH, cortisol, TSH, free T4)
- Dynamic endocrine testing as needed
- Ophthalmological evaluation:
- Visual field testing
- Visual acuity assessment
Imaging¶
- MRI (gold standard):
- T1-weighted:
- Isointense to gray matter
- Hypointense to white matter
- T2-weighted:
- Hyperintense to gray matter
- Contrast-enhanced T1:
- Heterogeneous enhancement
- Key features:
- Sellar expansion
- Suprasellar extension
- Cavernous sinus invasion (if present)
- CT:
- Hypodense to isodense mass
- Sellar expansion and remodeling
- Calcifications (in 5-25% of cases)
- Dedicated pituitary protocol:
- Thin-slice (1-3mm) coronal and sagittal images
- Dynamic contrast-enhanced sequences
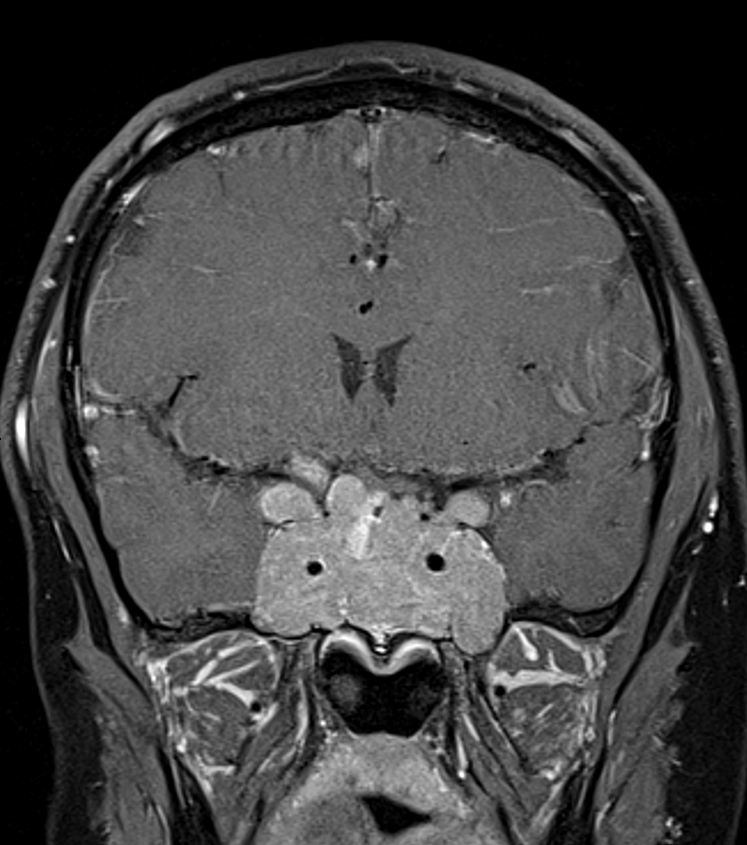
- 60-year-old patient with a large heterogeneously enhancing lesion within an expanded pituitary fossa. The optic chiasm is elevated and compressed.
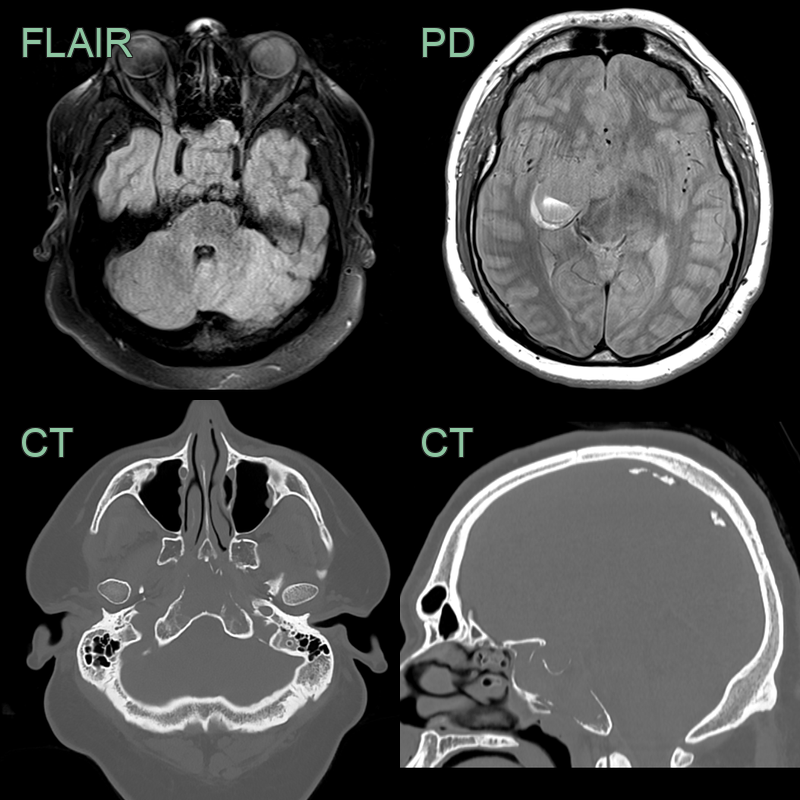
- 25-year-old patient presented with a seizure.
- MRI showed a large, enhancing (not shown) lesion centred in the pituitary fossa but with extensive erosion of the skull base.
- A hemtoma formed in the right lateral aspect of the lesion, the mass effect of which presumably provoked the seizure.
- Serum prolactin was >800,000. Prolactin levels and the size of the lesion significantly reduced after starting cabergoline.
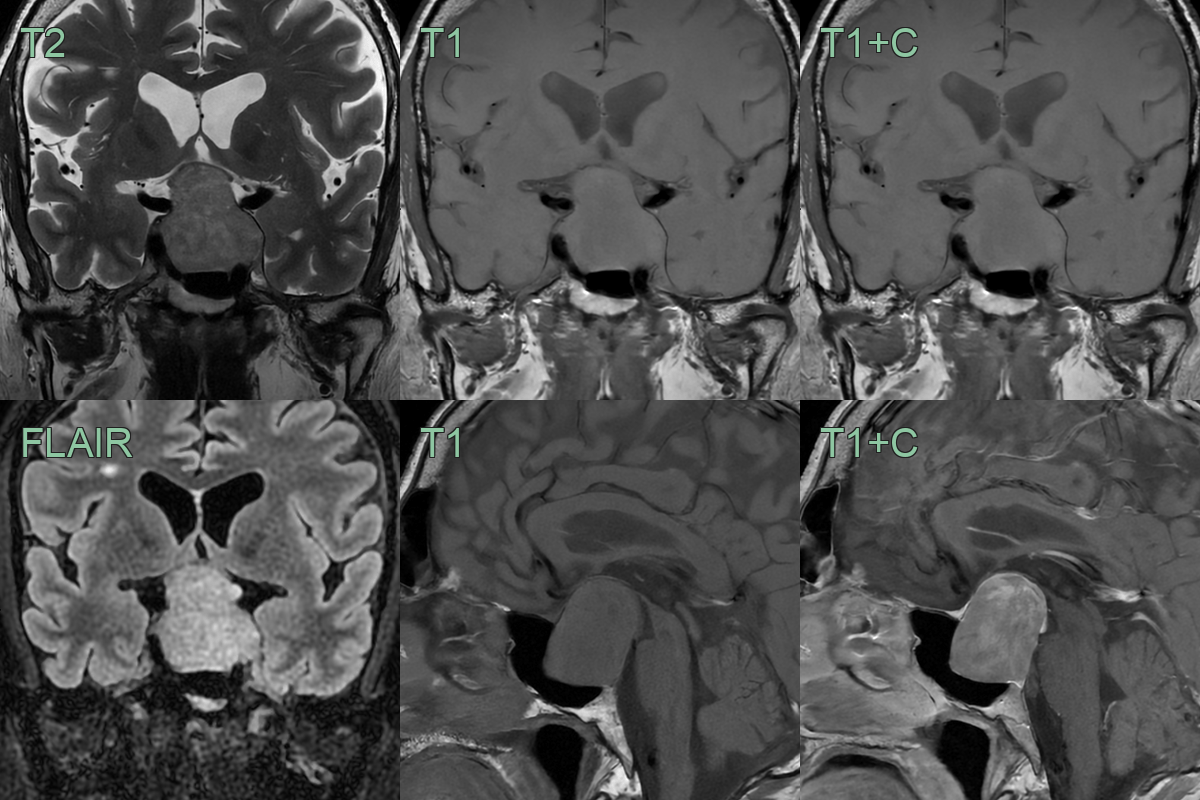
- 60-year-old patient presented with facial changes typical of acromegaly.
- MRI showed a 1.2 cm T2-hypointense lesion in the anterior aspect of the pituitary gland. The lesion was subtly hypoenhancing.
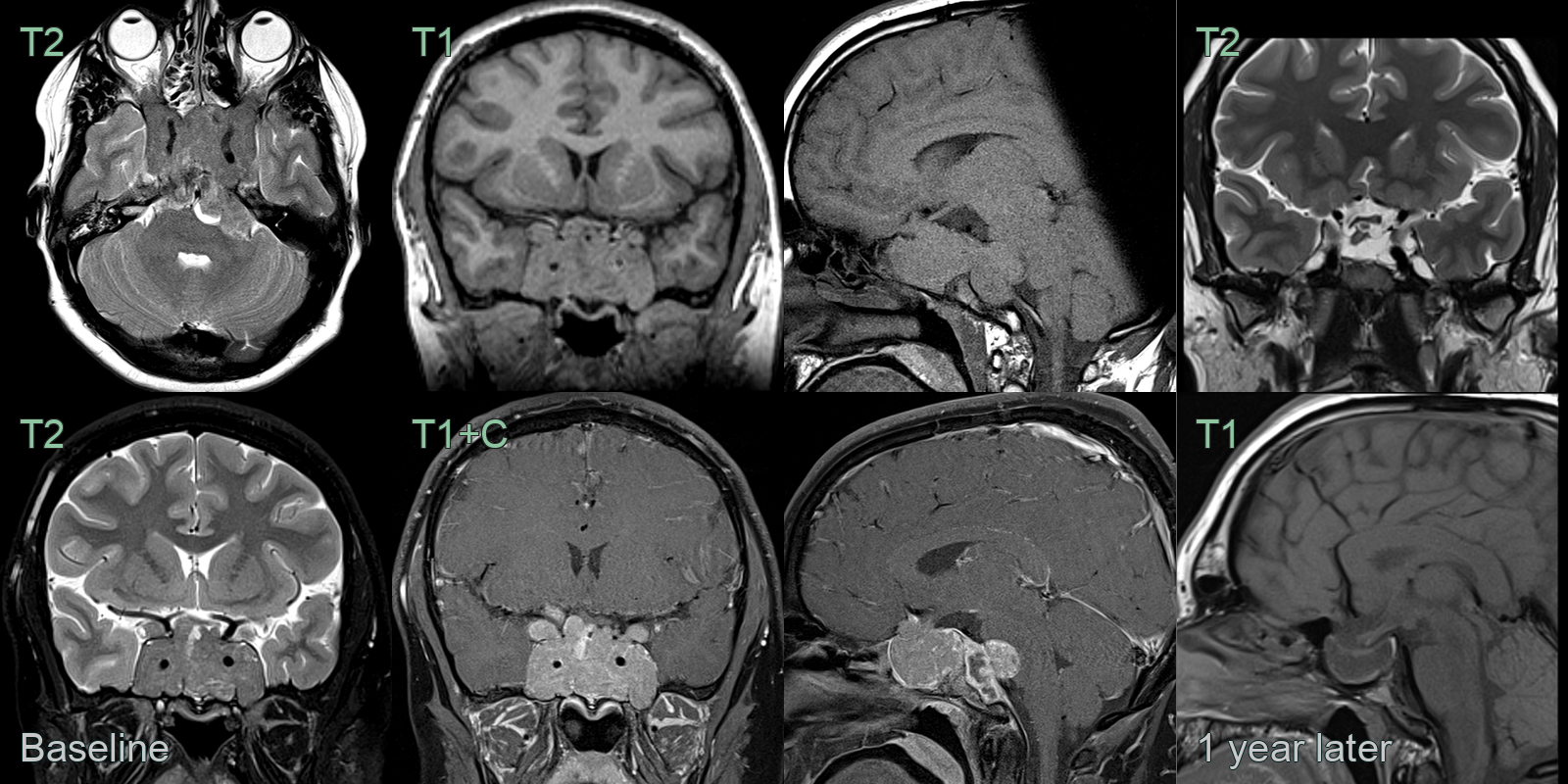
- A 25-year-old patient presented with headache and visual disturbance.
- MRI showed a massive skull base lesion centred on the pitutary fossa with involvement of the cavernous sinuses and extension along the clivus.
- After 1 year on cabergoline, the prolactinoma shrunk to a fraction of its original size.
Treatment¶
- Management approach depends on:
- Tumour size and extension
- Hormonal activity
- Patient's symptoms and comorbidities
- Surgical resection:
- Transsphenoidal approach (endoscopic or microscopic)
- Goals: Decompression, hormone normalization, tissue diagnosis
- Medical therapy:
- Prolactinomas: Dopamine agonists (e.g., cabergoline, bromocriptine)
- GH-secreting: Somatostatin analogs (e.g., octreotide, lanreotide)
- ACTH-secreting: Steroidogenesis inhibitors (e.g., ketoconazole)
- Radiation therapy:
- Reserved for residual or recurrent tumours
- Stereotactic radiosurgery or fractionated radiotherapy
- Hormonal replacement:
- For hypopituitarism due to tumour compression or treatment effects
- Regular follow-up:
- Serial MRI scans
- Endocrine evaluation
- Visual field testing
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Craniopharyngioma | Calcifications on CT; cystic components more common |
| Meningioma | Dural tail sign on MRI; homogeneous enhancement |
| Rathke's cleft cyst | Lack of solid component; thin wall enhancement |
| Metastasis | Irregular enhancement; bone destruction; posterior pituitary or infundibular predilection |
| Germ cell tumour | Midline pineal or suprasellar location; loss of posterior pituitary bright spot; thickened infundibulum |
| Chordoma | Destructive lesion of the clivus |