Polymicrogyria¶
Summary
- Polymicrogyria is a malformation of cortical development characterised by excessive small gyri and shallow sulci
- Results from abnormal neuronal migration and organization during fetal brain development
- Imaging shows thickened cortex with irregular gray-white matter junction and multiple small gyri
Pathophysiology¶
- Occurs due to disruption of late neuronal migration or early cortical organization (weeks 16-24 of gestation)
- Proposed mechanisms:
- Genetic mutations (e.g., GPR56, TUBB2B, PAX6)
- Intrauterine infections (e.g., cytomegalovirus, toxoplasmosis)
- Ischaemic insults during fetal development
- Results in abnormal cortical lamination and excessive small gyri formation
Demographics¶
- Prevalence estimated at 1 in 2500 live births
- No significant gender predilection
- Can occur in isolation or as part of genetic syndromes (e.g., 22q11.2 deletion syndrome)
Diagnosis¶
- Clinical presentation varies widely:
- Seizures (most common manifestation)
- Developmental delay
- Motor deficits
- Cognitive impairment
- Diagnosis primarily based on neuroimaging findings
- Genetic testing may be indicated in some cases
Imaging¶
- MRI is the modality of choice:
- T1-weighted images: Thickened cortex with irregular gray-white matter junction
- T2-weighted images: Multiple small gyri creating a "bumpy" cortical surface
- FLAIR: May show subcortical and deep white matter signal abnormalities
- Patterns of involvement:
- Focal: Affects a single lobe or region
- Multifocal: Multiple non-contiguous areas
- Diffuse: Bilateral and extensive involvement
- Common locations:
- Perisylvian region (most frequent)
- Frontal lobes
- Parietal lobes
- Associated findings:
- Ventriculomegaly
- Corpus callosum abnormalities
- Cerebellar dysplasia
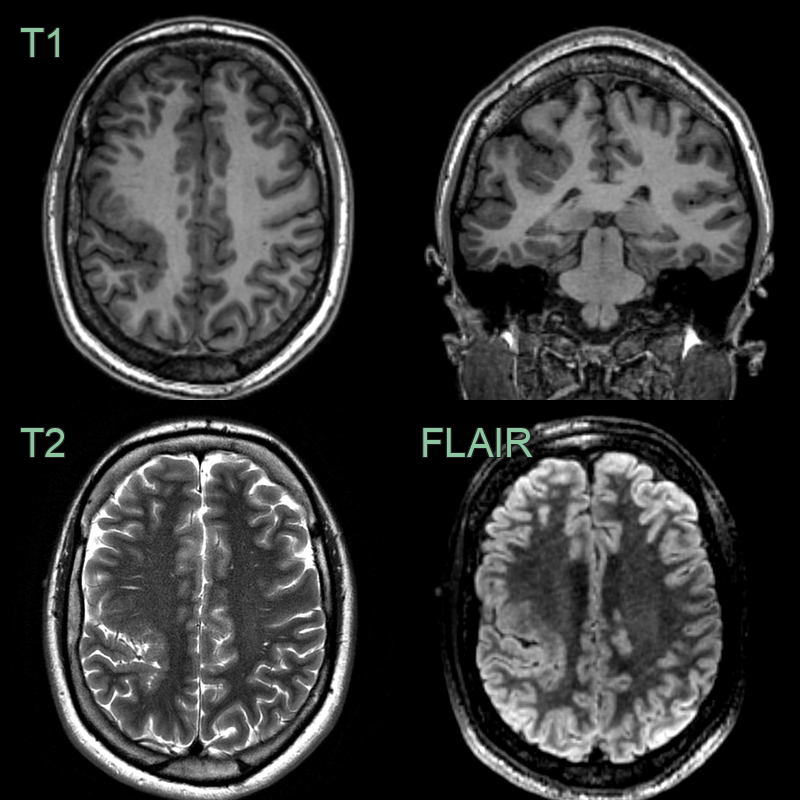
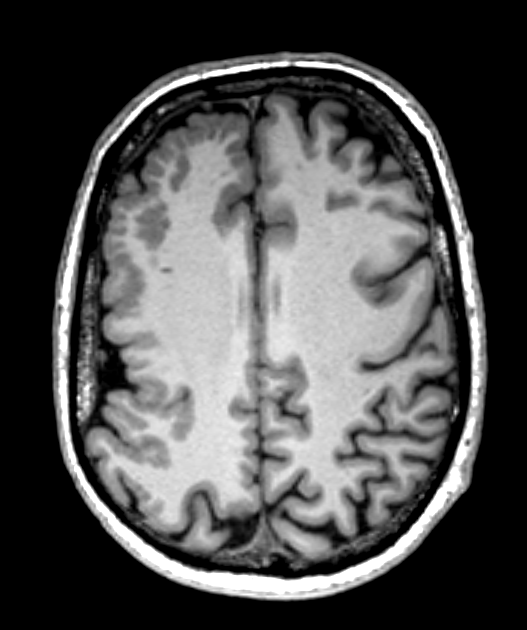
- 25-year-old patient with lifelong seizures.
- The cortex lining the right intraparietal sulcus was thickened and irregular.
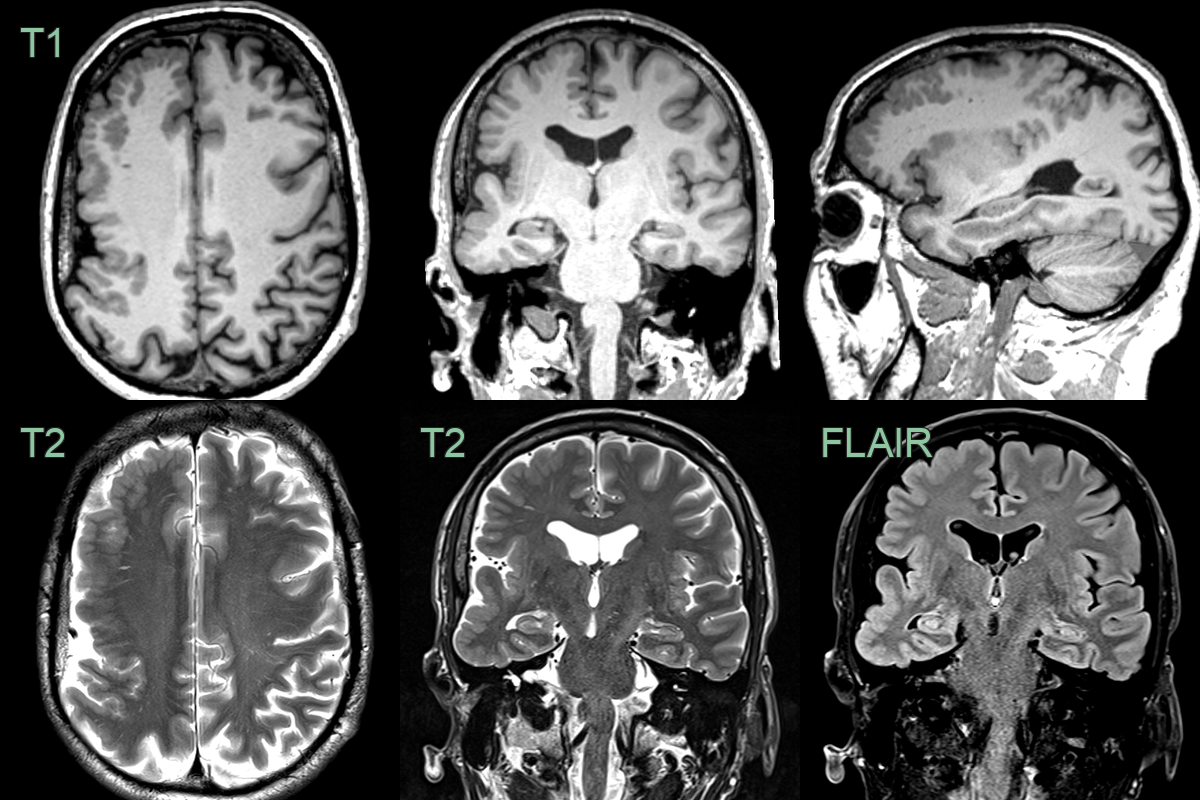
- A 50-year-old patient with a hemiplegia since birth presented with a possible seizure.
- MRI showed extensive polymicrogyria over the right cerebral hemisphere.
Treatment¶
- No curative treatment available
- Management focuses on symptom control:
- Antiepileptic drugs for seizure control
- Physical therapy for motor deficits
- Occupational and speech therapy for developmental delays
- Surgical interventions:
- Focal resection for intractable epilepsy in select cases
- Hemispherectomy for extensive unilateral involvement
- Genetic counseling for familial cases
- Regular follow-up to monitor developmental progress and manage complications
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Lissencephaly | Smooth brain surface without excessive gyri; polymicrogyria has numerous small gyri |
| Pachygyria | Broad, thick gyri; polymicrogyria has small, numerous gyri |
| Schizencephaly | Clefts extending from cortical surface to ventricles; not present in polymicrogyria |
| Focal cortical dysplasia | Focal cortical thickening and blurring of gray-white matter junction; polymicrogyria has more diffuse cortical involvement |
| Ulegyria | Mushroom-shaped gyri with preferential involvement of depths of sulci; polymicrogyria affects entire gyri |
| Perinatal hypoxic-ischaemic injury | Often bilateral and symmetric; polymicrogyria can be unilateral or asymmetric |
| Congenital cytomegalovirus infection | Periventricular calcifications often present; not typically seen in polymicrogyria |
| Tuberous sclerosis | Cortical/subcortical tubers and subependymal nodules; absent in polymicrogyria |
| Zika virus infection | Subcortical calcifications and ventriculomegaly; not typical features of polymicrogyria |