Posterior Cortical Atrophy (PCA)¶
Summary
- Neurodegenerative syndrome characterised by progressive decline in visual processing and other posterior cortical functions
- Typically presents with visual complaints despite intact primary visual pathways
- Imaging shows atrophy of parietal, occipital, and occipitotemporal cortices
Pathophysiology¶
- Underlying pathology is most commonly Alzheimer's disease (AD) in 80-100% of cases
- Other causes include:
- Dementia with Lewy bodies
- Corticobasal degeneration
- Prion disease
- Selective vulnerability of posterior brain regions, particularly visual association areas
- Neuronal loss and accumulation of amyloid plaques and neurofibrillary tangles in affected areas
Demographics¶
- Typically affects individuals in their 50s or 60s
- Mean age of onset: 58-60 years
- No clear gender predilection
- Rare disorder, estimated to account for 5-10% of early-onset dementia cases
Diagnosis¶
- Clinical presentation:
- Progressive visual dysfunction (e.g., difficulty reading, recognising objects, or navigating)
- Preserved memory and insight in early stages
- Later development of other cognitive deficits
- Neuropsychological testing:
- Impairments in visuospatial and visuoperceptual tasks
- Relatively preserved memory and language functions
- Diagnostic criteria:
- Proposed by Crutch et al. (2017)
- Core features include insidious onset, gradual progression, and prominent visual deficits
Imaging¶
- Structural MRI:
- Atrophy of parietal, occipital, and occipitotemporal cortices
- Relative sparing of medial temporal lobes and hippocampi in early stages
- Progressive atrophy with disease progression
- Functional imaging (PET/SPECT):
- Hypometabolism/hypoperfusion in posterior cortical regions
- Asymmetry common, with right hemisphere often more affected
- Advanced techniques:
- Diffusion tensor imaging: white matter tract degeneration in posterior regions
- Amyloid PET: positive in AD-related PCA cases

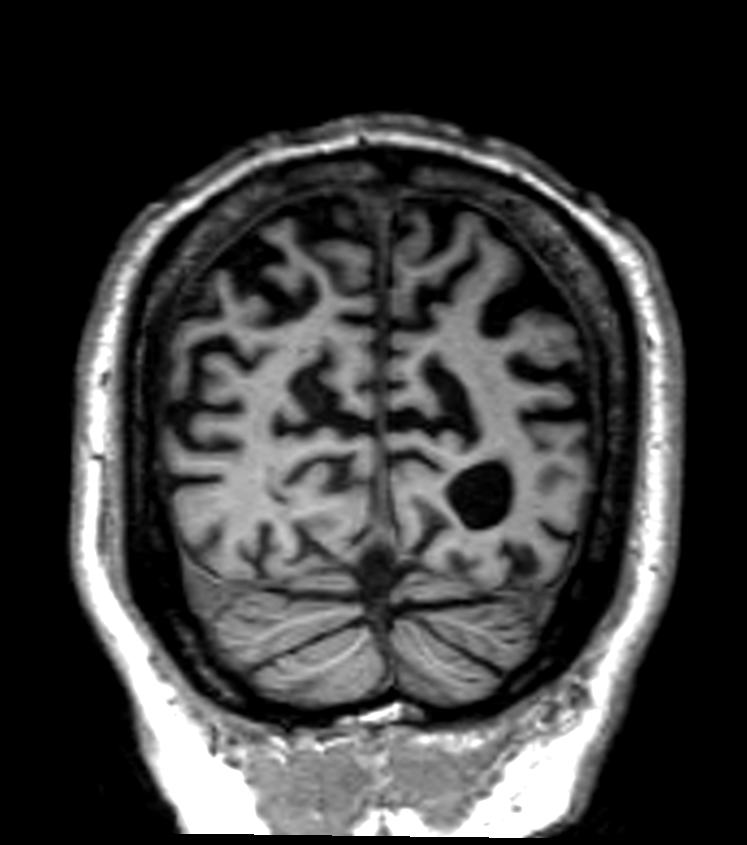
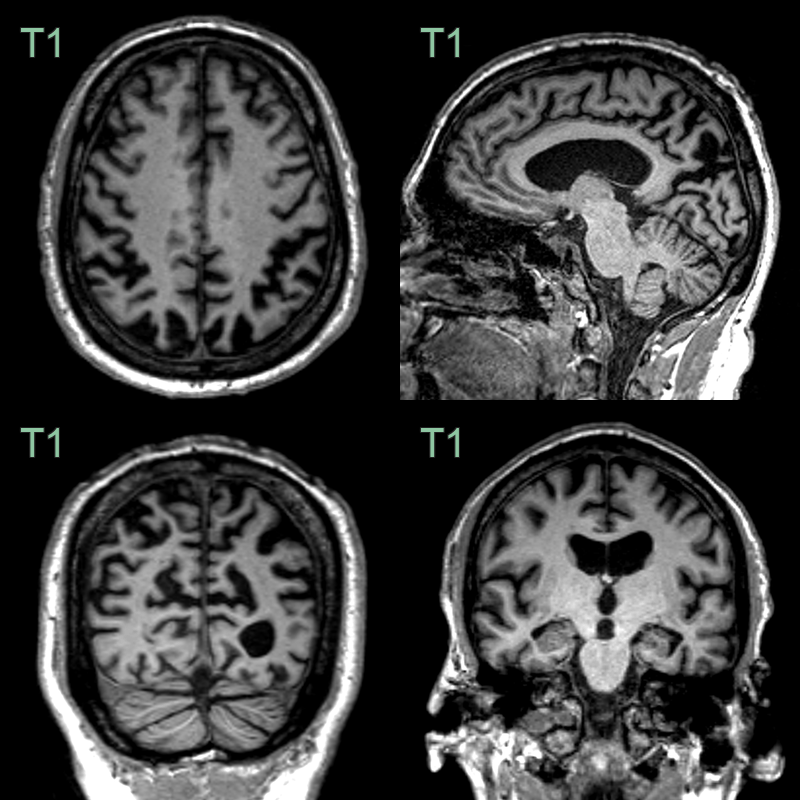
- A 65-year-old patient presented with memory impairment, visual hallucinations and apraxia.
- MRI showed relatively mild hippocampal atrophy on the right but severe symmetrical atrophy of the parietal and occipital lobes.
- CSF biomarkers were compatible with Alzheimer's disease.
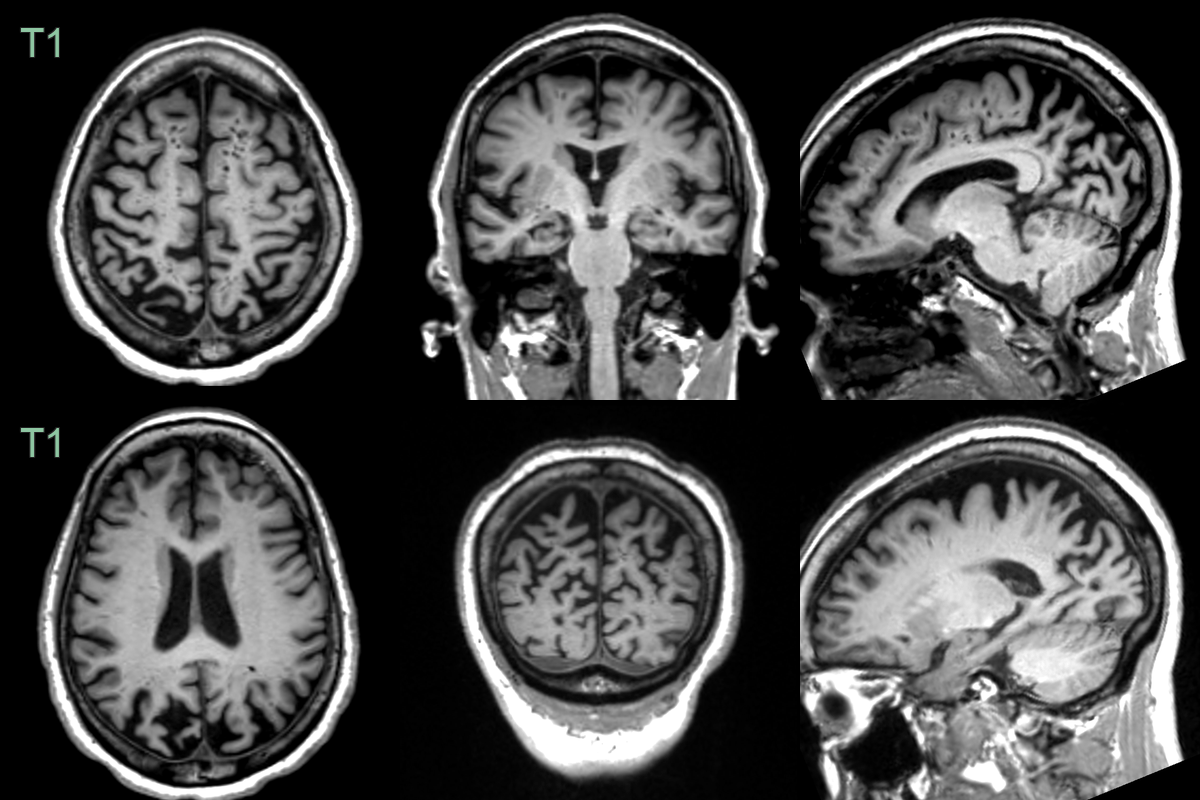
- A 60-year-old patient presented with logopenic aphasia and memory impairment.
- MRI showed marked widening of parietal and, to a lesser extent, occipital sulci.
- Hippocampal volume loss was less pronounced (MTAS 2).
- CSF biomarkers were consistent with Alzheimer's disease.
Treatment¶
- No disease-modifying treatments currently available
- Symptomatic management:
- Acetylcholinesterase inhibitors (e.g., donepezil) may provide modest cognitive benefit
- Memantine for moderate to severe cases
- Non-pharmacological interventions:
- Occupational therapy to address visual and spatial deficits
- Environmental modifications to improve safety and function
- Cognitive rehabilitation strategies
- Support and education for patients and caregivers
- Regular monitoring and adjustment of care plan as disease progresses