Primary CNS lymphoma¶
Summary
- Rare, aggressive non-Hodgkin lymphoma confined to the CNS
- Typically presents with focal neurological deficits, cognitive changes, or seizures
- Characteristic imaging findings include homogeneous enhancement and restricted diffusion
Pathophysiology¶
- Most cases are diffuse large B-cell lymphomas (DLBCL)
- Arises from malignant transformation of lymphocytes within the CNS
- Exact etiology unknown, but associated with immunosuppression (e.g., HIV, organ transplantation)
- Disruption of blood-brain barrier allows for tumour growth and invasion
Demographics¶
- Accounts for 1-2% of all non-Hodgkin lymphomas
- Median age at diagnosis: 65 years
- Male to female ratio: 1.2-1.7:1
- Higher incidence in immunocompromised individuals
Diagnosis¶
- Clinical presentation:
- Focal neurological deficits (70%)
- Neuropsychiatric symptoms (43%)
- Increased intracranial pressure (33%)
- Seizures (14%)
- Laboratory findings:
- CSF analysis: elevated protein, low glucose, lymphocytic pleocytosis
- Serum LDH often elevated
- Definitive diagnosis:
- Stereotactic brain biopsy
- Flow cytometry and immunohistochemistry to confirm B-cell origin
Imaging¶
- CT:
- Hyperdense lesions with moderate to marked enhancement
- Minimal surrounding oedema
- MRI:
- T1: hypointense to isointense
- T2/FLAIR: iso to hyperintense
- Diffusion-weighted imaging: restricted diffusion
- Contrast-enhanced T1:
- Homogeneous enhancement
- "Butterfly" pattern in corpus callosum lesions
- PET/CT:
- High FDG uptake in lesions
- Useful for staging and treatment response assessment
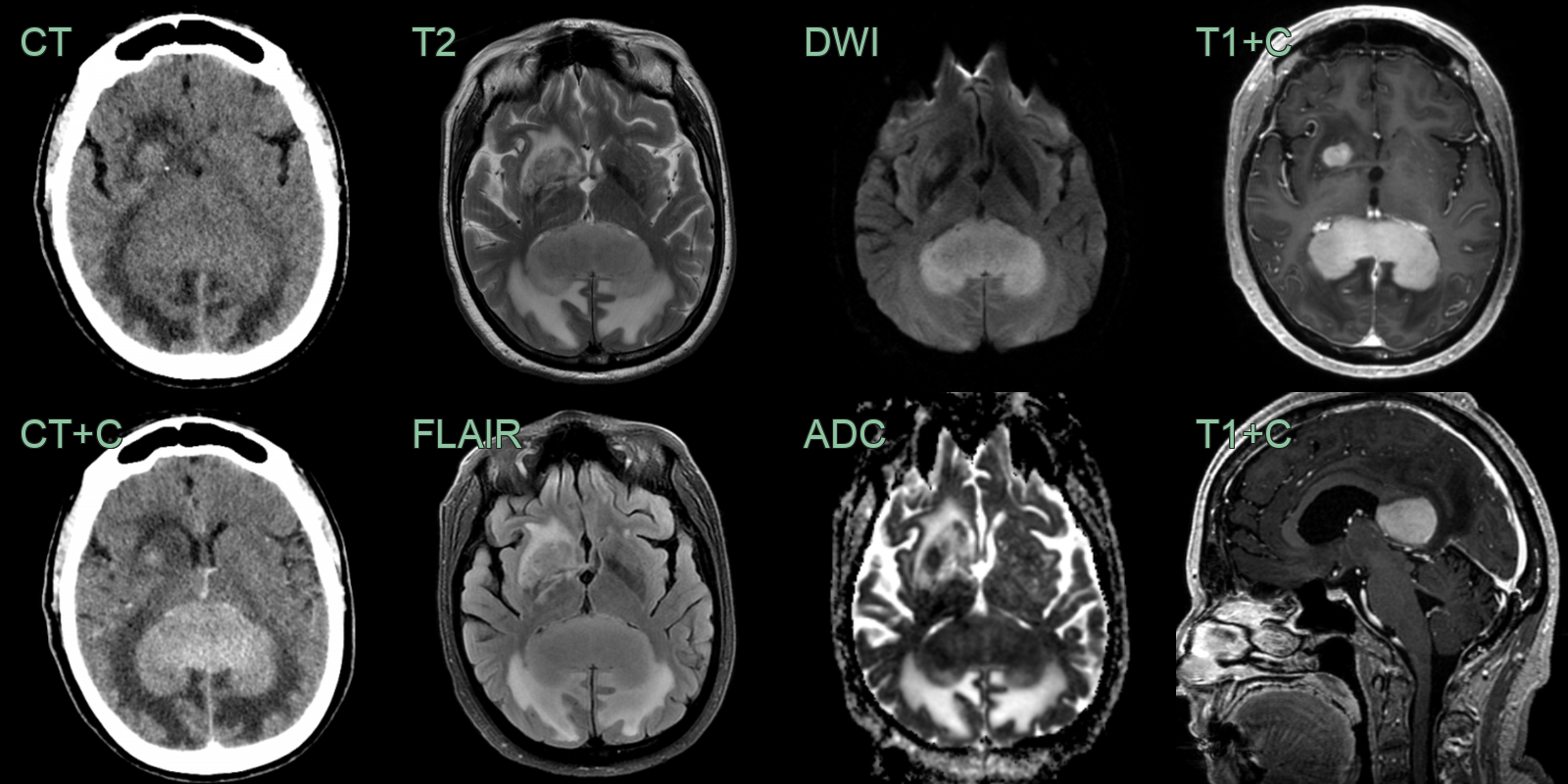
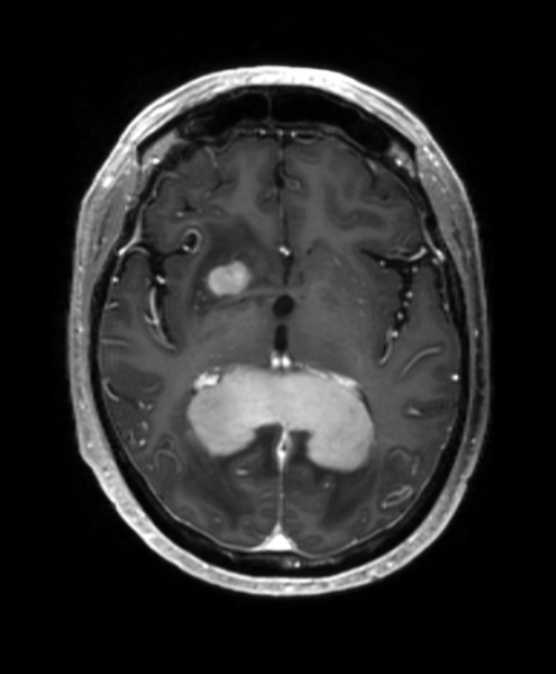
- 70-year-old patient presented with a 3 week history of headaches.
- CT showed a grossly enlarged and subtly hyperattenuating splenium.
- On MRI, the lesion enhanced homogeneously with diffusion restriction.
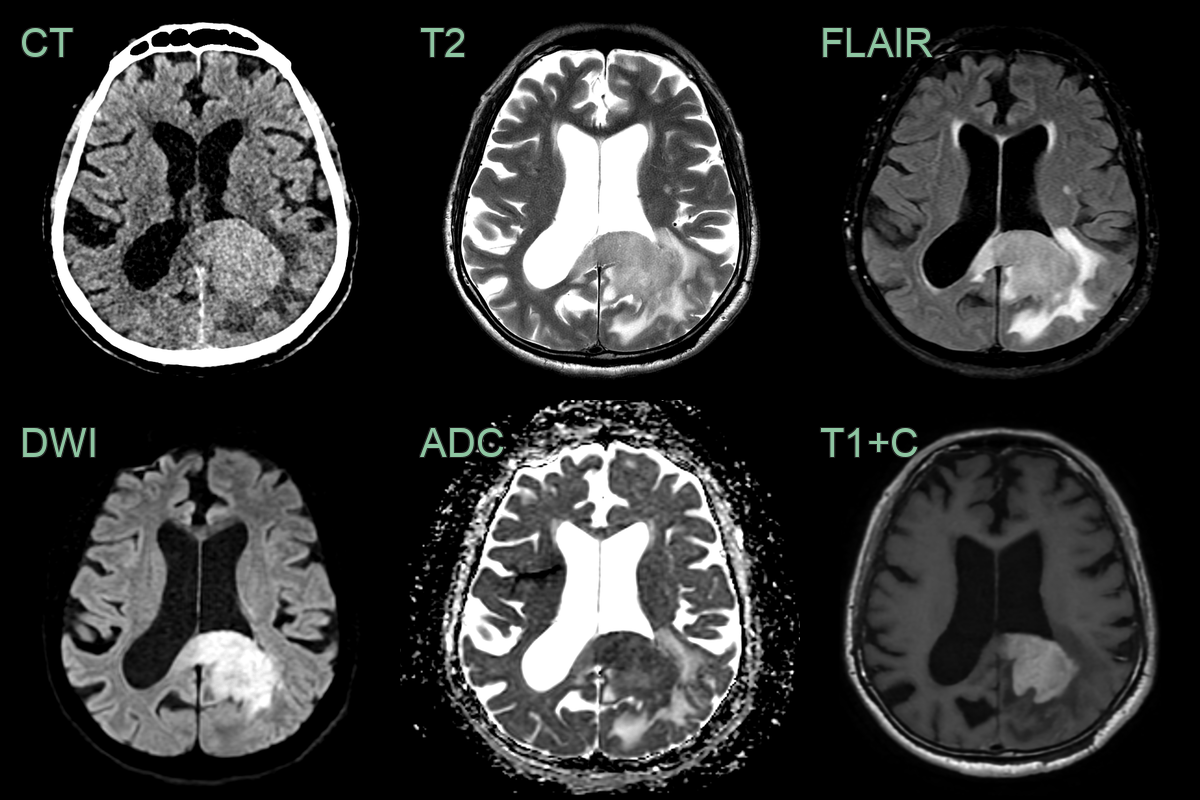
- A 70-year-old patient presented with confusion and visual disturbance.
- CT showed a hyperdense lesion involving the parietal white matter and corpus callosum.
- Relative hypointensity on T2 and low values on ADC also indicated hypercellularity.
- Alongside confluent avid enhancement, the imaging was typical for the final diagnosis of PCNSL.
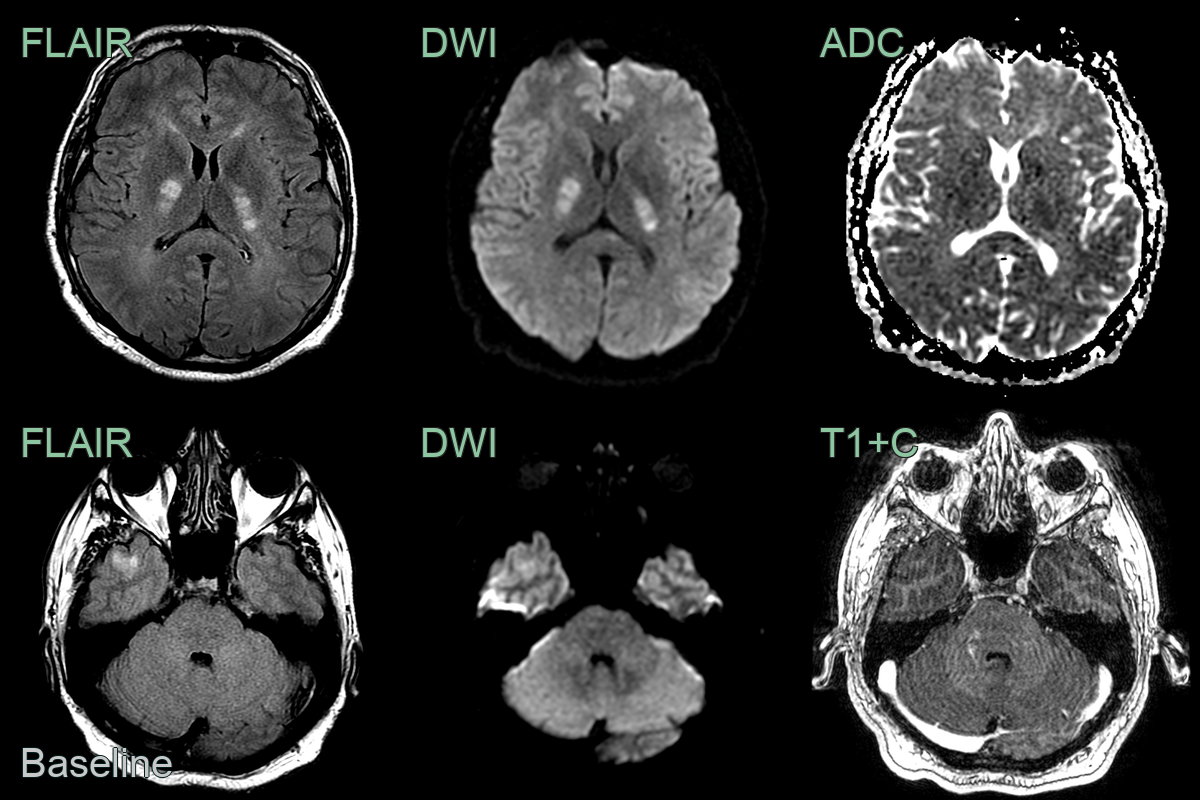
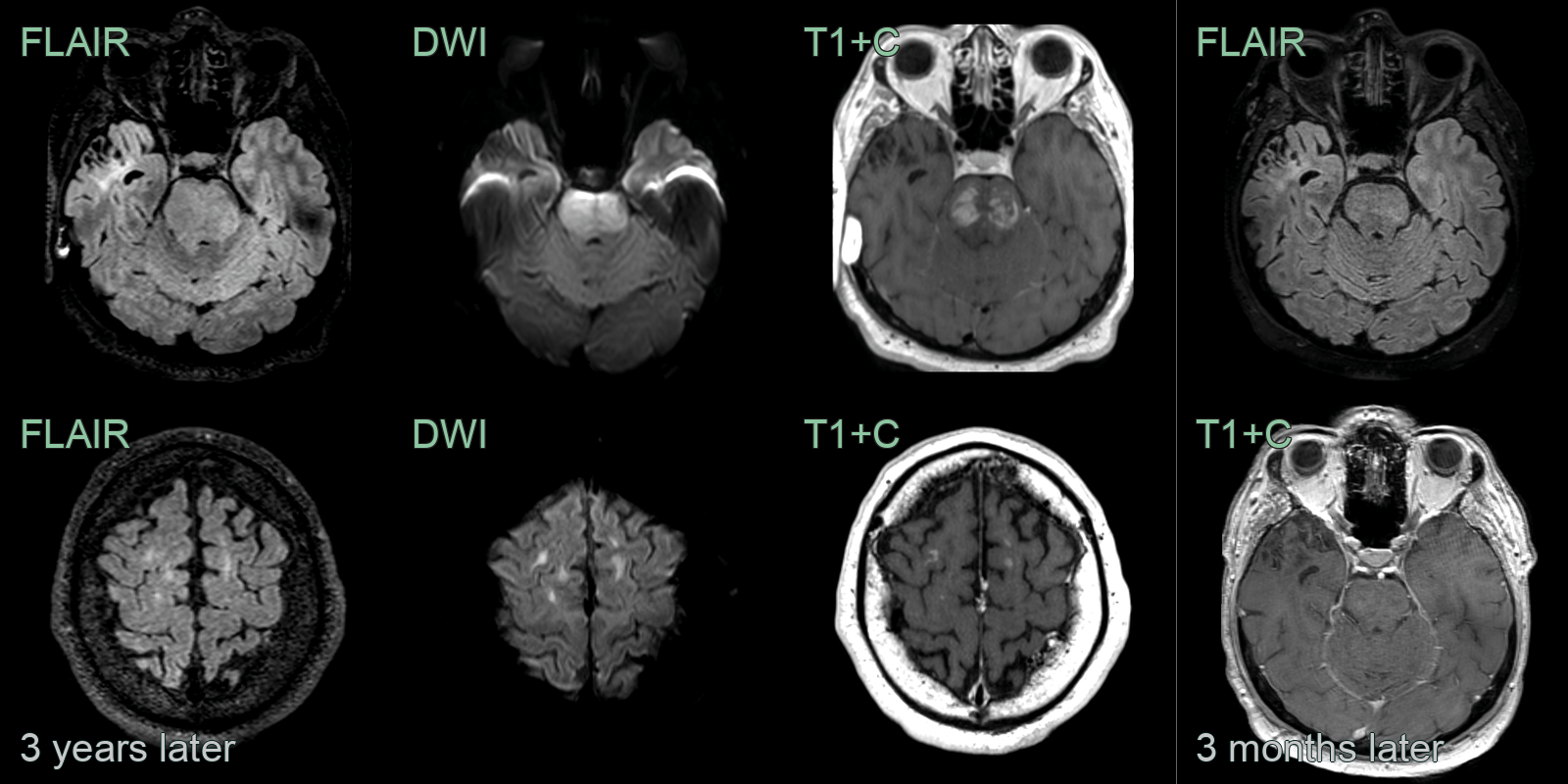
- A 40-year-old patient presented with agitation and aggressive behaviour.
- MRI showed mutliple lesions, some of which caused diffusion restriction (internal capsules) and some of which enhanced (right hemipons).
- A diagnosis was not secured even after extensive investigation. The lesions responded to a trial of steroid therapy.
- 3 years later, the patient presented following a seizure. MRI showed marked progression with an infiltative and enhancing lesion in the brainstem and new frontal lobe lesions.
- Biopsy of a right frontal lesion revealed a diffuse large B-cell lymphoma, which again showed a response to therapy.
Treatment¶
- High-dose methotrexate-based chemotherapy:
- First-line treatment
- Often combined with rituximab
- Whole-brain radiation therapy:
- Reserved for patients who cannot tolerate chemotherapy
- Associated with significant neurotoxicity
- Targeted therapies:
- Ibrutinib (BTK inhibitor) shows promise in relapsed/refractory cases
- Stem cell transplantation:
- Considered for younger, fit patients with chemosensitive disease
- Supportive care:
- Corticosteroids for cerebral oedema
- Anticonvulsants for seizure control
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Glioblastoma | Typically has more heterogeneous enhancement and necrosis on MRI |
| Metastatic brain tumour | Often multiple lesions at the grey-white matter junction; ring or nodular enhancement; surrounding vasogenic oedema |
| Toxoplasmosis | Ring-enhancing lesions in basal ganglia and at grey-white matter junction; restricted diffusion in centre |
| Multiple sclerosis | Typically smaller lesions, periventricular distribution |
| Acute disseminated encephalomyelitis | More diffuse, bilateral, asymmetric white matter involvement; grey matter involvement common; no restricted diffusion typically |
| Cerebral abscess | Ring-enhancing lesion with restricted diffusion on DWI |
| Subacute infarct | Follows arterial vascular territory; gyral enhancement pattern; no restricted diffusion in subacute phase |
| Tumefactive demyelination | Incomplete ("open ring") enhancement pattern; less mass effect relative to lesion size; no DWI restriction |
| Neurosarcoidosis | Leptomeningeal and perivascular enhancement; cranial nerve involvement; no corpus callosum or periventricular predilection |
| Progressive multifocal leukoencephalopathy | Asymmetric subcortical white matter lesions without enhancement; U-fibre involvement; no mass effect |