Progressive Multifocal Leukoencephalopathy (PML)¶
Summary
- PML is a rare, often fatal demyelinating disease of the central nervous system caused by reactivation of the JC virus in immunocompromised individuals
- Characterised by multifocal areas of demyelination in the white matter
- Imaging typically shows asymmetric, multifocal white matter lesions without mass effect or enhancement
Pathophysiology¶
- Caused by reactivation of latent JC virus in immunocompromised hosts
- Virus infects oligodendrocytes, leading to demyelination
- Predominantly affects subcortical white matter, with occasional involvement of grey-white matter junction
- Lesions typically progress and coalesce over time
Demographics¶
- Rare disease, with an incidence of 0.2 cases per 100,000 person-years
- Most commonly affects:
- HIV/AIDS patients (80% of cases)
- Patients with hematological malignancies
- Organ transplant recipients
- Patients on immunosuppressive therapies (e.g., natalizumab for multiple sclerosis)
Diagnosis¶
- Clinical presentation:
- Cognitive decline
- Motor deficits
- Visual disturbances
- Seizures
- Cerebrospinal fluid analysis:
- JC virus PCR (sensitivity 72-92%, specificity 92-100%)
- Brain biopsy (gold standard, but rarely performed)
- Neuroimaging plays a crucial role in diagnosis and follow-up
Imaging¶
- MRI is the modality of choice
- Typical findings:
- Asymmetric, multifocal white matter lesions
- Subcortical and periventricular predilection
- Hypointense on T1-weighted images
- Hyperintense on T2-weighted and FLAIR sequences
- No mass effect or surrounding oedema
- Minimal or no enhancement (10-15% may show faint peripheral enhancement)
- Advanced techniques:
- Diffusion-weighted imaging: restricted diffusion in acute lesions
- MR spectroscopy: decreased NAA, increased choline and lipid peaks
- Perfusion imaging: typically shows hypoperfusion in affected areas
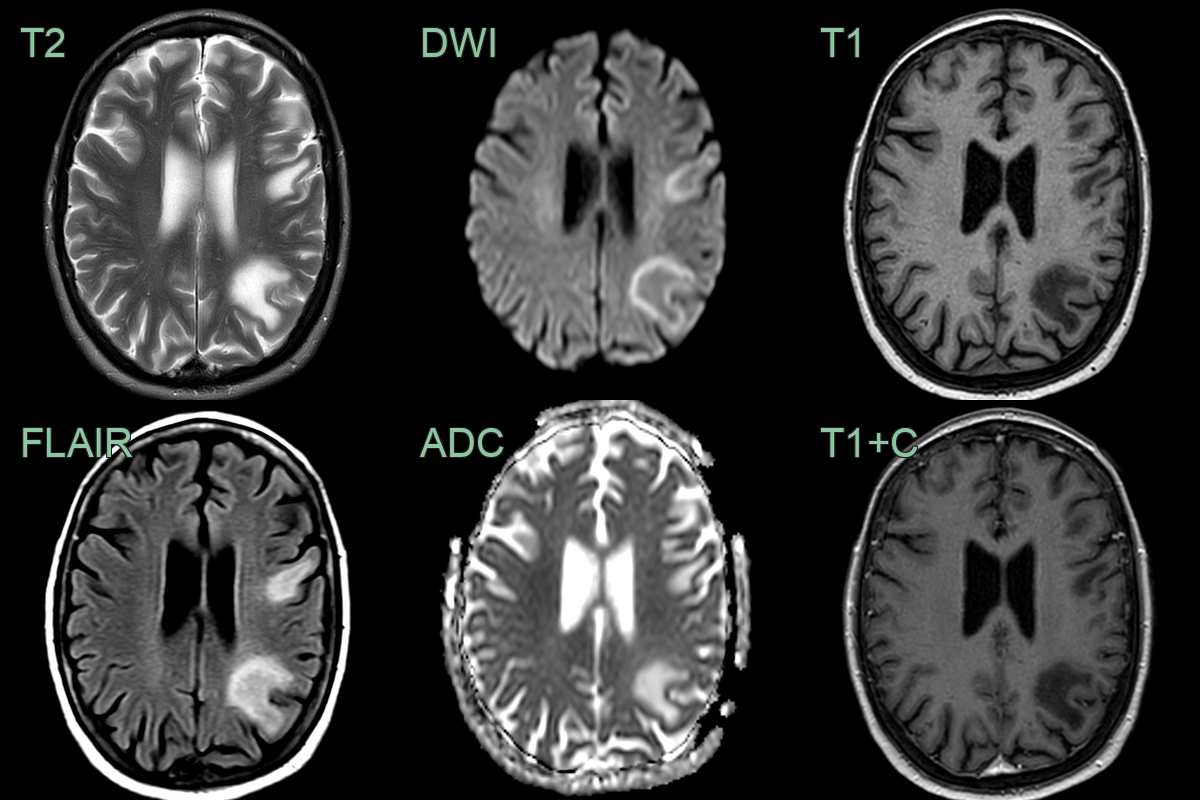
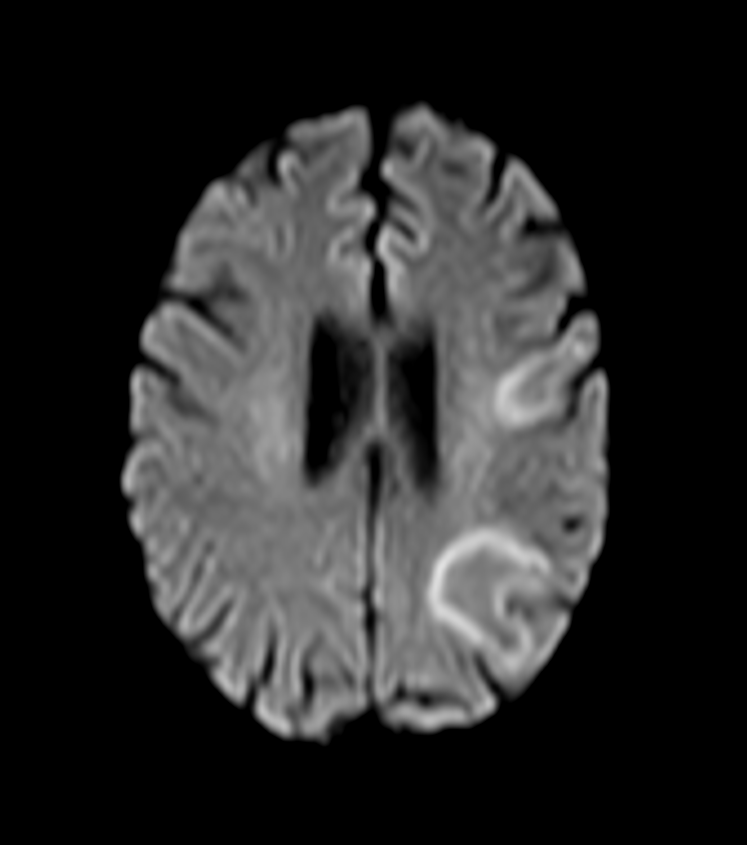
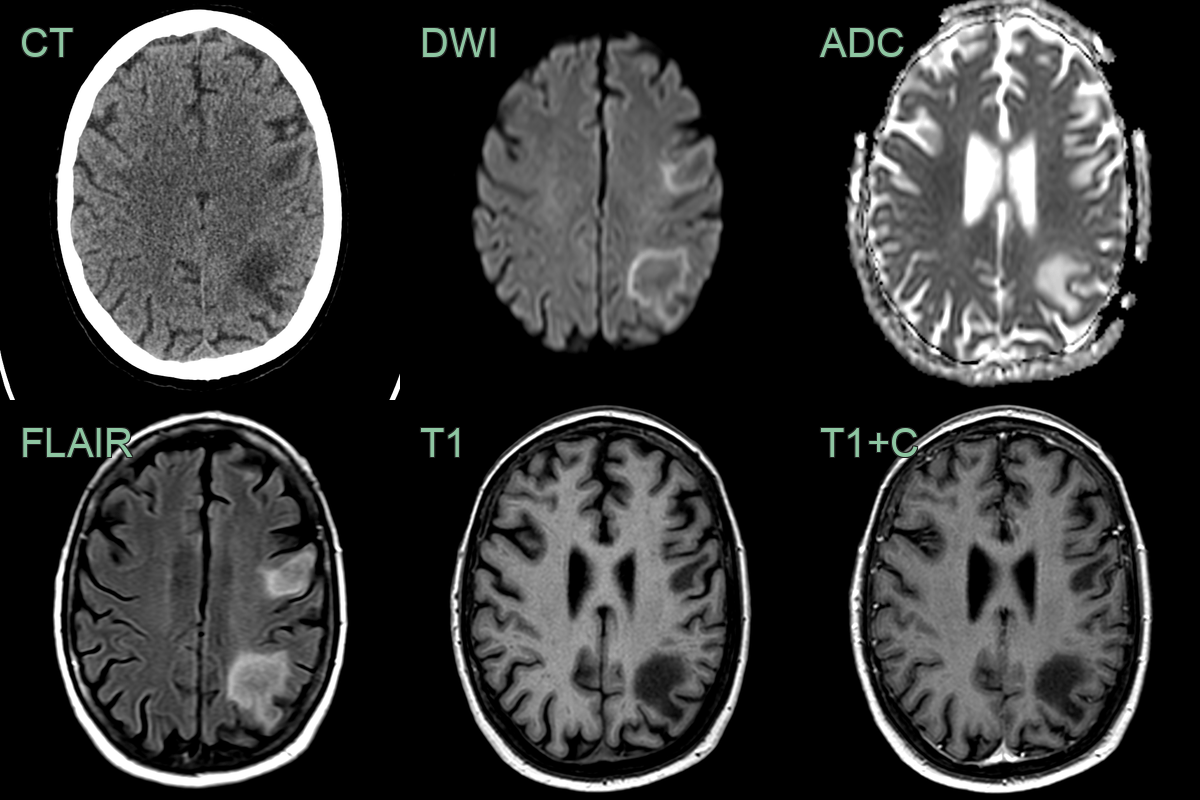
- A 70-year-old patient, who was undergoing chemotherapy for thyroid cancer, presented with a change in personality and right sided weakness.
- MRI showed multifocal subcortical T2-weighted hyperintensity with a rim of diffusion restriction and no enahncement.
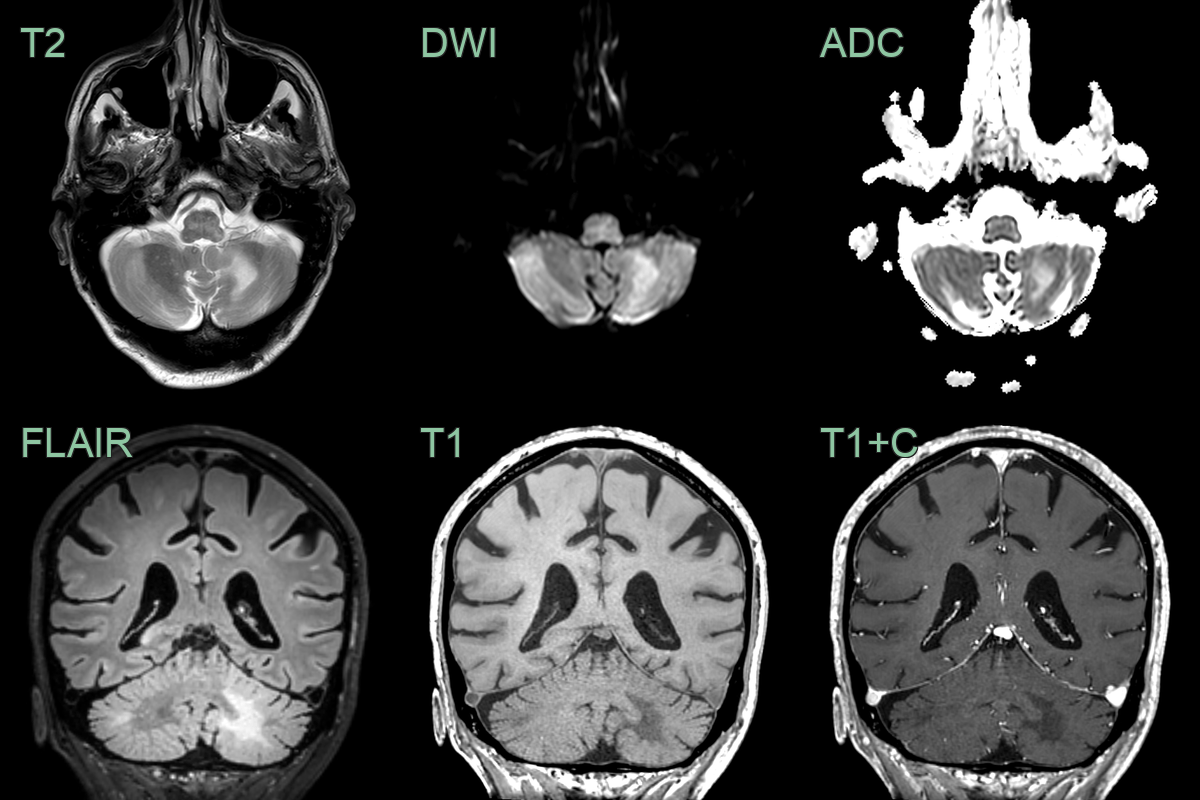
- 75-year-old patient on immunosuppression for rhematoid arthritis presented with subacute cerebellar ataxia.
- MRI showed a T2 and diffusion-weighted hyperintensity in the cerebellar white matter without enhancement.
- JC virus was positive and the lesions regressed after cessation of immunosuppressants.
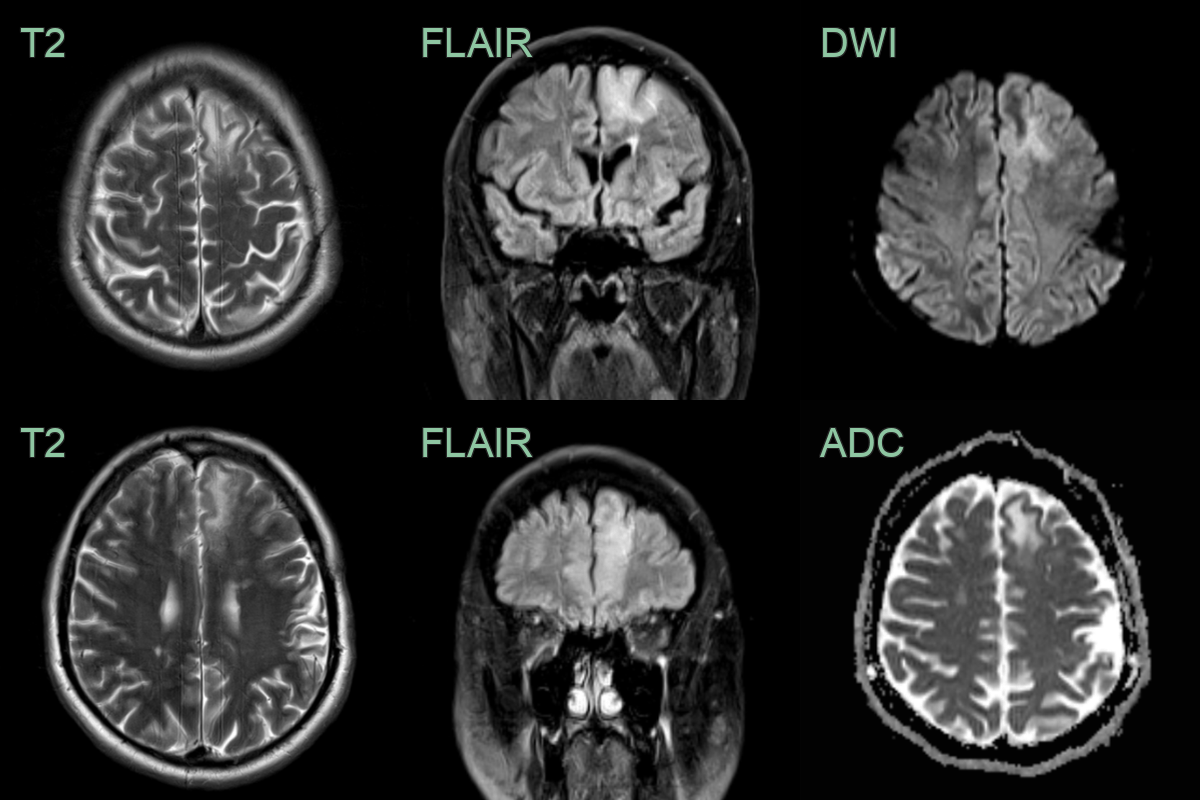
- 60-year-old patient on long term immunosuppression for rheumatoid arthritis presented following a seizure.
- MRI showed left frontal white matter hyperintensity extending into the juxtacortical white matter with no mass effect or diffusion restriction.
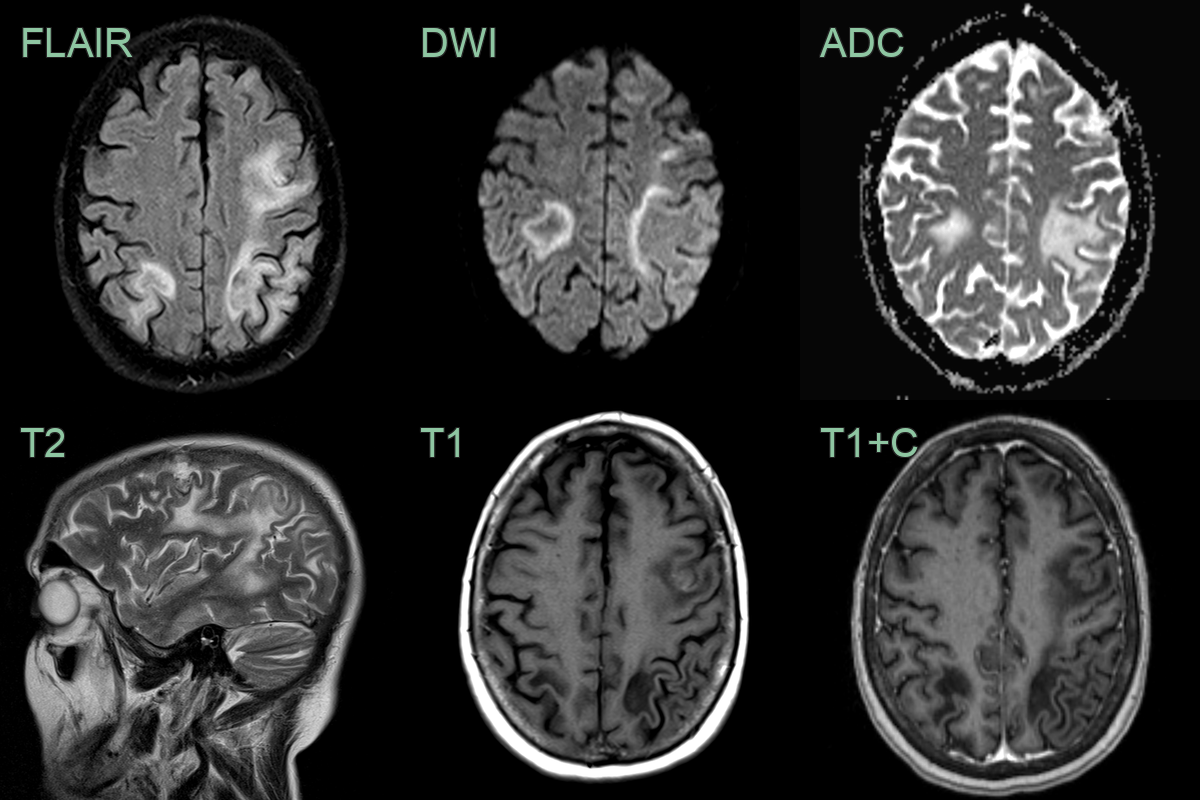
- 70-year-old patient undergoing treatment for lymphoma. Presented with seizures, confusion, and aphasia.
- MRI showed peripheral FLAIR-hyperintense and T1-hypointense lesions extending up to the cortex with no mass effect or enhancement.
- After one month and treatment with pembrolizumab, the lesions had enlarged with a more obvious leading edge of diffusion weighted hyperintensity. There was no contrast enhancement to suggest PML-IRIS.
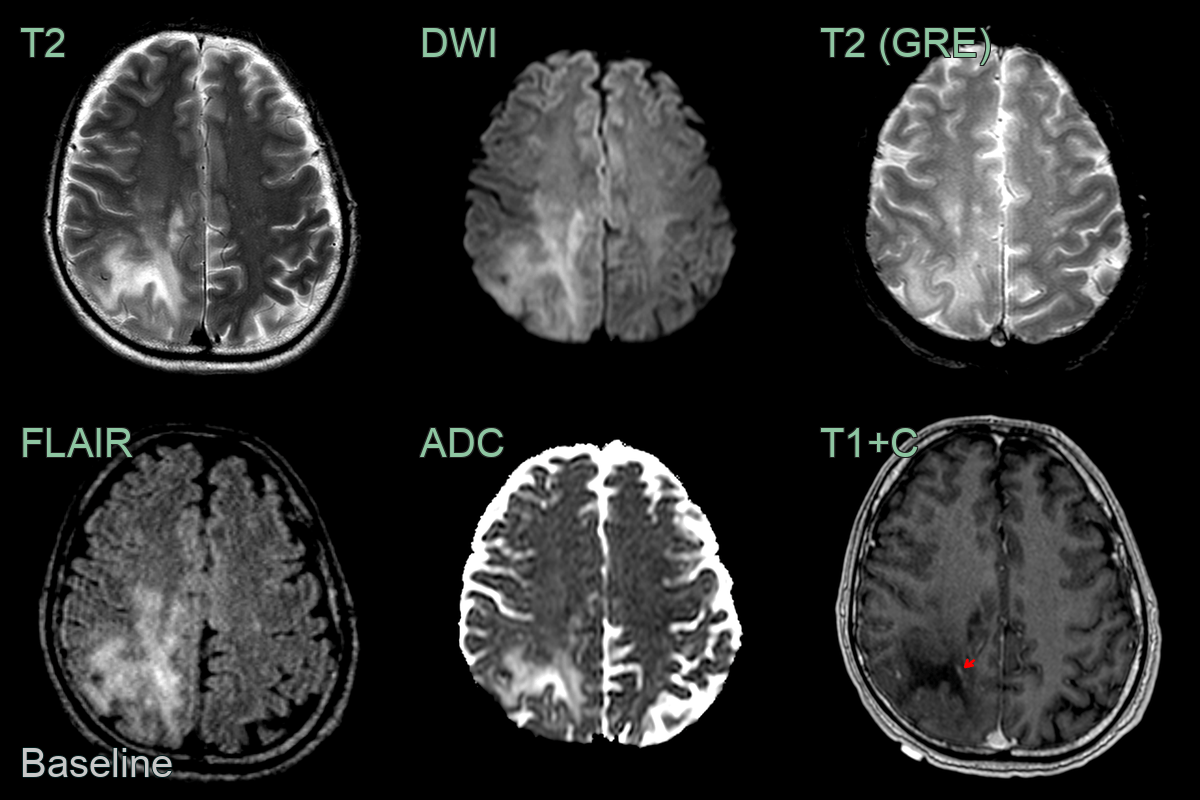
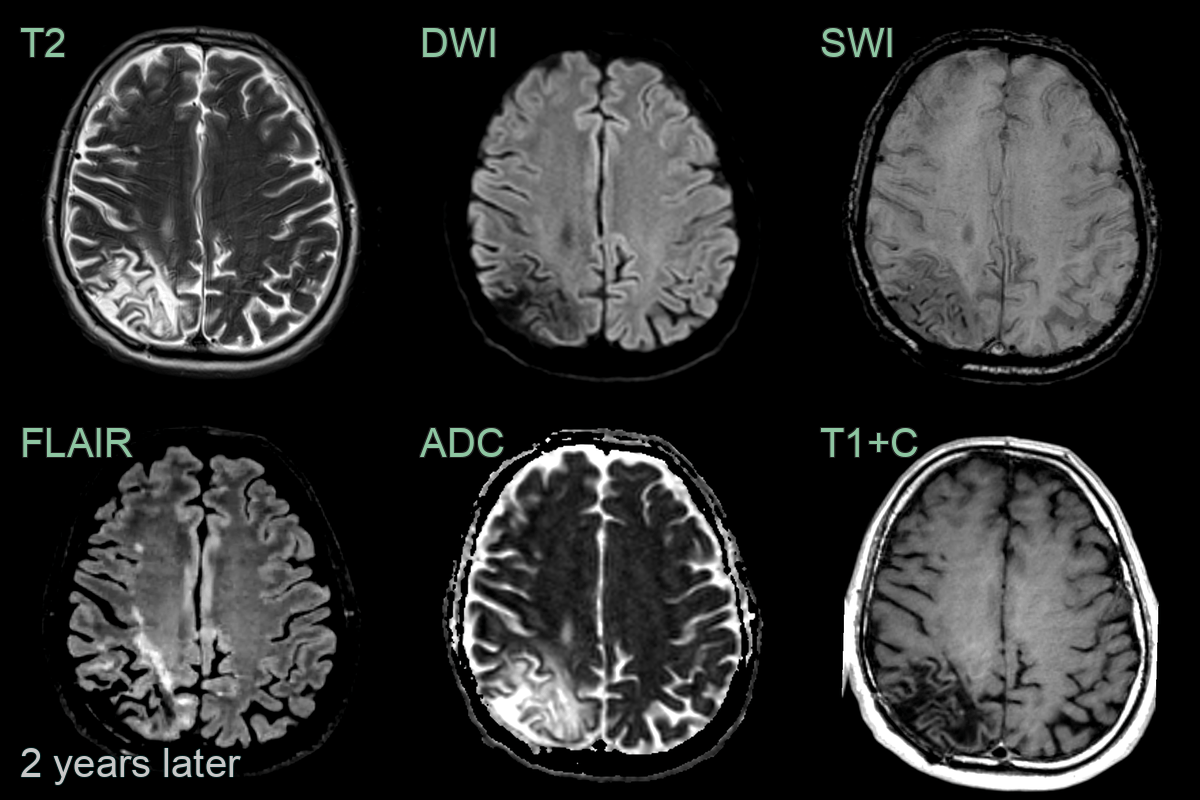
- A 40-year-old patient who had recently underwent CAR-T treatment for lymphoma presented after a 2 week history of headache and photophobia.
- MRI showed a large confluent subcortical region of T2-hyperintensity with a subtle rim of relative diffusion restriction and enhancement.
- Biopsy confirmed PML.
- On follow-up imaging 2 years later, following successful remission of lymphoma, the region matured into a region of gliosis.
Treatment¶
- No specific antiviral therapy available
- Management focuses on immune reconstitution:
- HIV patients: optimisation of antiretroviral therapy
- Withdrawal or reduction of immunosuppressive medications when possible
- Supportive care and management of complications
- Experimental therapies:
- Cidofovir (limited evidence of efficacy)
- Mefloquine (clinical trials ongoing)
- Immune checkpoint inhibitors (case reports of success in some patients)
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Multiple Sclerosis | Ovoid periventricular and calloso-septal interface lesions (Dawson fingers); well-defined borders; subcortical U-fibres spared |
| Acute Disseminated Encephalomyelitis | Bilateral asymmetric lesions involving both grey and white matter; lesions typically enhance; basal ganglia involvement common |
| Primary CNS Lymphoma | Tends to enhance with contrast; often periventricular |
| HIV Encephalopathy | More diffuse white matter involvement; typically spares U-fibres |
| Cerebral Toxoplasmosis | Ring-enhancing lesions; often affects basal ganglia |
| Stroke | Follows arterial vascular territory; DWI restriction in acute phase with ADC corresponding signal; no subcortical U-fibre predilection |
| Posterior Reversible Encephalopathy Syndrome | Posterior cortical and subcortical vasogenic oedema; ADC map elevated (not restricted); involves grey and white matter |
| Glioblastoma | Usually single, large enhancing mass; significant mass effect |
| Metastatic Brain Tumours | Multiple lesions at grey-white matter junction; ring or nodular enhancement; surrounding vasogenic oedema |
| Cryptococcosis | Predilection for basal ganglia; meningeal involvement common |