Radiation Induced Cerebral Vasculopathy¶
Summary
- Delayed complication of cranial radiation therapy
- Characterised by progressive narrowing and occlusion of cerebral blood vessels
- Imaging findings include white matter changes, vessel stenosis, and moyamoya-like collaterals
Pathophysiology¶
- Radiation-induced damage to vascular endothelium
- Accelerated atherosclerosis and intimal hyperplasia
- Fibrinoid necrosis of small vessels
- Increased production of pro-inflammatory cytokines and growth factors
- Impaired vascular remodeling and repair mechanisms
Demographics¶
- Incidence: 12-50% of patients receiving cranial radiation therapy
- Risk factors:
- Higher radiation doses (>50 Gy)
- Younger age at time of radiation exposure
- Concomitant chemotherapy
- Pre-existing vascular risk factors (e.g., hypertension, diabetes)
Diagnosis¶
- Clinical presentation:
- Typically occurs 1-30 years post-radiation therapy
- Headaches, cognitive decline, focal neurological deficits
- Transient ischaemic attacks or stroke-like episodes
- Laboratory findings:
- Elevated inflammatory markers (e.g., ESR, CRP)
- Normal cerebrospinal fluid analysis
Imaging¶
- Magnetic Resonance Imaging (MRI):
- T2/FLAIR hyperintensities in periventricular and subcortical white matter
- Lacunar infarcts and microbleeds
- Cortical atrophy and ventricular enlargement
- Magnetic Resonance Angiography (MRA):
- Stenosis or occlusion of large intracranial arteries
- Moyamoya-like collateral vessel formation
- Computed Tomography Angiography (CTA):
- Vessel wall thickening and luminal narrowing
- Calcifications in affected vessels
- Digital Subtraction Angiography (DSA):
- Gold standard for evaluating vascular changes
- Demonstrates extent of stenosis and collateral circulation
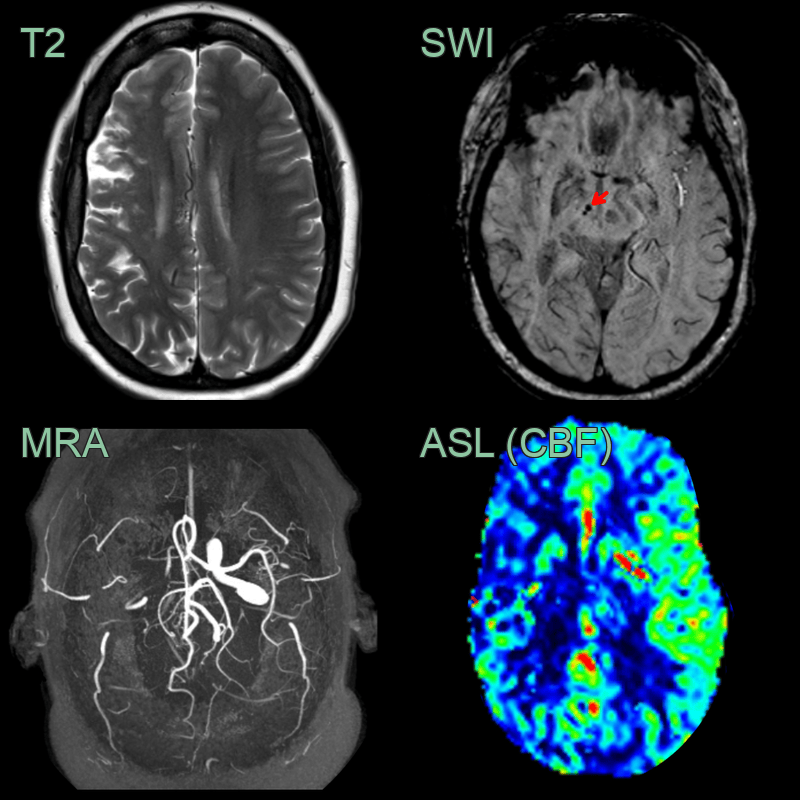
- A 40-year-old patient received radioetherapy to treat a posterior arteriovenous malformation in childhood.
- There were old superficial borderzone territory infarcts in the right cerebral convexity as well as a few microhaemorrhages (red arrow).
- MRA showed severe stenosis of the right terminal ICA, MCA and PCA.
- ASL showed reduced perfusion in the right MCA and, to a lesser extent, PCA territory.
Treatment¶
- Medical management:
- Antiplatelet therapy (e.g., aspirin)
- Control of vascular risk factors
- Neuroprotective agents (e.g., memantine)
- Surgical interventions:
- Direct or indirect revascularization procedures
- Extracranial-intracranial bypass surgery
- Endovascular treatments:
- Angioplasty and stenting for focal stenosis
- Intra-arterial vasodilator therapy
- Supportive care:
- Cognitive rehabilitation
- Management of seizures and headaches
- Experimental therapies:
- Hyperbaric oxygen therapy
- Stem cell therapies for vascular regeneration
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Atherosclerosis | Calcified plaques in vessel walls on CT; diffuse large vessel involvement not confined to a single anatomical region; no moyamoya-like collaterals |
| CADASIL | FLAIR hyperintensity with anterior temporal pole and external capsule predilection; subcortical lacunar infarcts; no large vessel stenosis or cavernomas |
| Primary CNS vasculitis | "String of beads" alternating narrowing and dilatation on conventional angiography; multifocal infarcts in multiple vascular territories; vessel wall enhancement on high-resolution MRI |
| Moyamoya disease | Bilateral ICA terminus and proximal MCA/ACA occlusion; "puff of smoke" lenticulostriate collaterals on DSA; basal ganglia and thalamic involvement |
| Reversible cerebral vasoconstriction syndrome | Multifocal cerebral artery vasoconstriction reversible on follow-up MRA; posterior leukoencephalopathy pattern; no vessel wall thickening |
| Cerebral amyloid angiopathy | Lobar microbleeds in posterior predominant distribution (parieto-occipital); cortical superficial siderosis on SWI; not confined to a focal anatomical region |
| Hypertensive microangiopathy | Deep microbleeds in basal ganglia, thalami, and brainstem; diffuse periventricular white matter changes; not confined to a focal region |