Rathke's cleft cyst¶
Summary
- Benign, non-neoplastic sellar/suprasellar lesion
- Derived from remnants of Rathke's pouch
- Typically asymptomatic; may cause headaches, visual disturbances, or endocrine dysfunction
Pathophysiology¶
- Originates from remnants of Rathke's cleft, an embryological structure
- Lined by ciliated columnar or cuboidal epithelium
- Contains proteinaceous fluid, mucoid material, or cellular debris
- May enlarge over time due to fluid accumulation or haemorrhage
Demographics¶
- Prevalence: 12-33% in autopsy studies
- More common in females (F:M ratio 2:1)
- Can occur at any age, but typically diagnosed in adults (30-50 years)
- Rare in children and adolescents
Diagnosis¶
- Often incidental finding on imaging studies
- Clinical presentation (if symptomatic):
- Headaches
- Visual disturbances (e.g., bitemporal hemianopsia)
- Endocrine dysfunction (e.g., hyperprolactinemia, hypopituitarism)
- Differential diagnosis:
- Craniopharyngioma
- Pituitary adenoma
- Arachnoid cyst
- Cystic pituitary apoplexy
Imaging¶
- MRI:
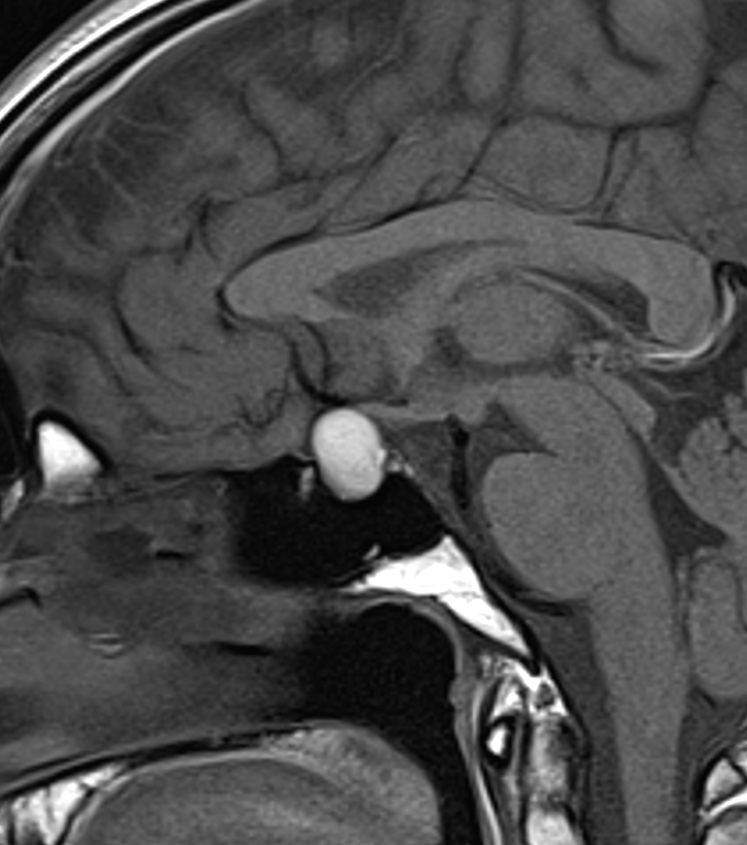
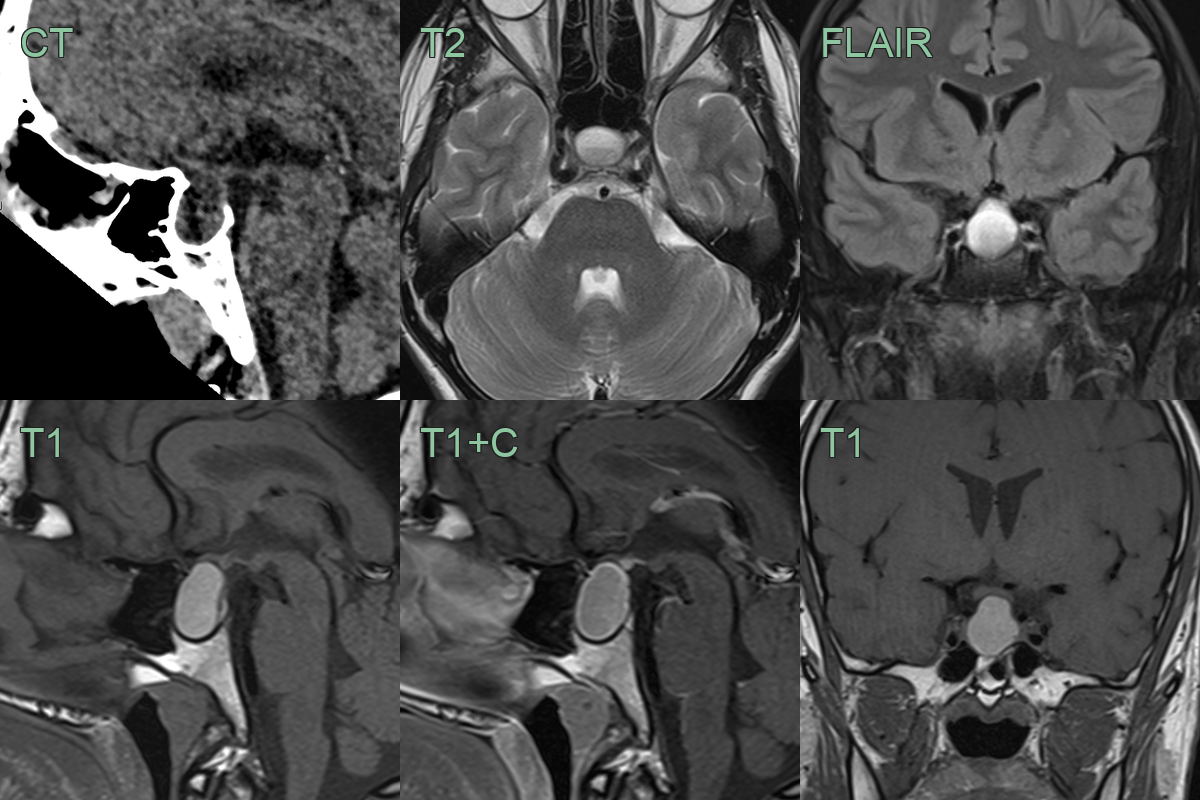
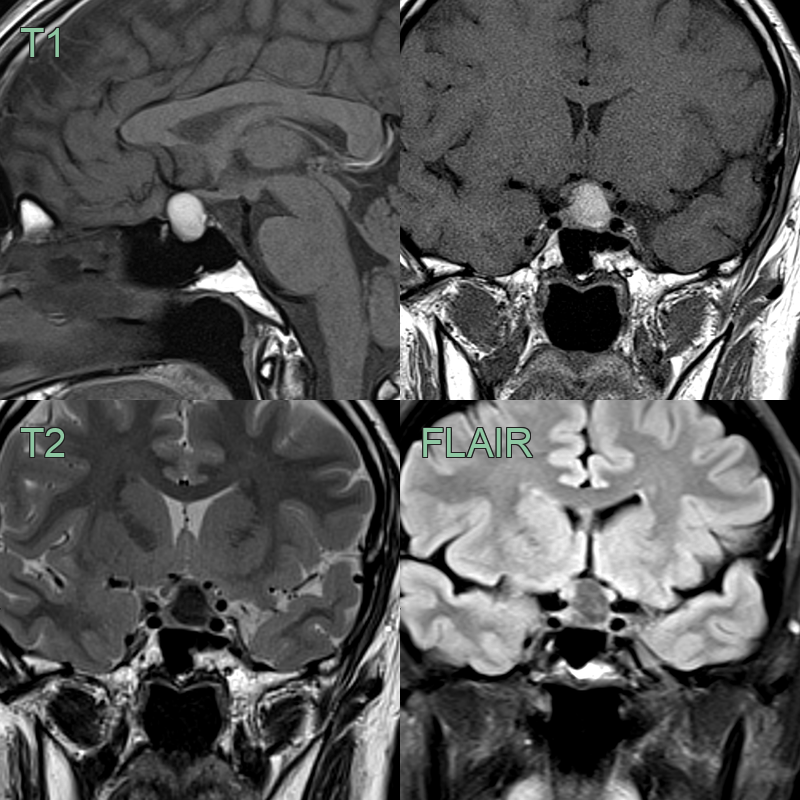
- T1-weighted: Variable signal intensity (dependent on protein content)
- T2-weighted: Typically hyperintense
- No enhancement with gadolinium (wall may enhance if inflamed)
- "Waxy" appearance on T2-weighted images
- CT:
- Hypodense cystic lesion
- Calcifications rare (unlike craniopharyngiomas)
- Key features:
- Well-defined, smooth margins
- No solid component
- Lack of calcification
- 30-year-old patient had imaging after a road traffic accident.
- An incidental sellar-suprasellar lesion that was T1 hyperintense and T2-hypointense was consistent with a Rathke's cleft cyst.
- Other than fluctuting changes in internal signal intensity, the lesion had not changed in over a 5 year period.
- Despite mass effect on the chiasm, there has been no visual impairment.
Treatment¶
- Asymptomatic cases:
- Observation with serial imaging
- Endocrine function monitoring
- Symptomatic cases:
- Surgical intervention:
- Transsphenoidal approach (most common)
- Transcranial approach (for large suprasellar extension)
- Goals: Cyst drainage, partial wall resection
- Postoperative management:
- Hormone replacement therapy if needed
- Follow-up imaging to assess for recurrence
- Recurrence rate: 5-10%
- Radiation therapy: Generally not recommended due to benign nature
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Craniopharyngioma | Calcifications on CT; solid or mixed solid-cystic components; suprasellar predominance |
| Cystic pituitary adenoma | Typically off-midline; may show septations or fluid-fluid level; solid enhancement on contrast MRI |
| Arachnoid cyst | Follows CSF signal on all sequences including FLAIR suppression; no wall enhancement |
| Cystic pituitary apoplexy | Haemorrhagic T1 hyperintensity within the lesion; fluid-fluid level; gland enlargement |
| Epidermoid cyst | Restricted diffusion on DWI with low ADC values; more irregular margins |
| Dermoid cyst | Fat signal on T1 and T2 with chemical shift artefact; may show fat-fluid level |
| Teratoma | Mixed solid and cystic components; fatty signal on T1; may calcify |
| Colloid cyst | Located at foramen of Monro in anterior third ventricle; hyperdense on CT |
| Metastasis | Solid or rim-enhancing sellar mass; posterior pituitary or infundibular involvement |
| Aneurysm | Flow voids on MRI; pulsation artefacts; confirms on angiography |