Reversible Cerebral Vasoconstriction Syndrome (RCVS)¶
Summary
- RCVS is characterised by severe thunderclap headaches and reversible multifocal cerebral arterial constriction
- Typically affects women aged 20-50 years
- Diagnosis relies on clinical presentation, exclusion of other causes, and neuroimaging findings
Pathophysiology¶
- Exact mechanism unclear, but involves transient dysregulation of cerebral vascular tone
- Proposed triggers:
- Sympathetic overactivity
- Endothelial dysfunction
- Oxidative stress
- Associated with:
- Vasoactive substances (e.g., serotonergic drugs, cannabis)
- Postpartum state
- Migraine
Demographics¶
- Predominantly affects women (F:M ratio 2-10:1)
- Peak incidence: 20-50 years of age
- Rare in children and elderly
Diagnosis¶
- Clinical features:
- Sudden-onset, severe 'thunderclap' headaches
- Nausea, vomiting, photophobia
- Focal neurological deficits (in some cases)
- Diagnostic criteria (International Classification of Headache Disorders-3):
- Acute severe headache, often thunderclap-like
- Multifocal segmental vasoconstriction of cerebral arteries
- No evidence of aneurysmal subarachnoid haemorrhage
- Normal or near-normal CSF analysis
- Complete or substantial normalisation of arteries within 3 months
Imaging¶
- CT brain:
- Initially normal in most cases
- May show subarachnoid haemorrhage, intracerebral haemorrhage, or ischaemic infarction in complicated cases
- CT angiography:
- 'String of beads' appearance of cerebral arteries
- Multifocal segmental narrowing of cerebral arteries
- MRI brain:
- T2/FLAIR: may show vasogenic oedema, especially in posterior regions
- DWI: may reveal acute ischaemic changes
- MR angiography:
- Similar findings to CT angiography
- Useful for follow-up imaging to demonstrate reversibility
- Digital subtraction angiography:
- Gold standard for diagnosis
- Shows characteristic multifocal segmental arterial constriction
- Useful when non-invasive imaging is inconclusive
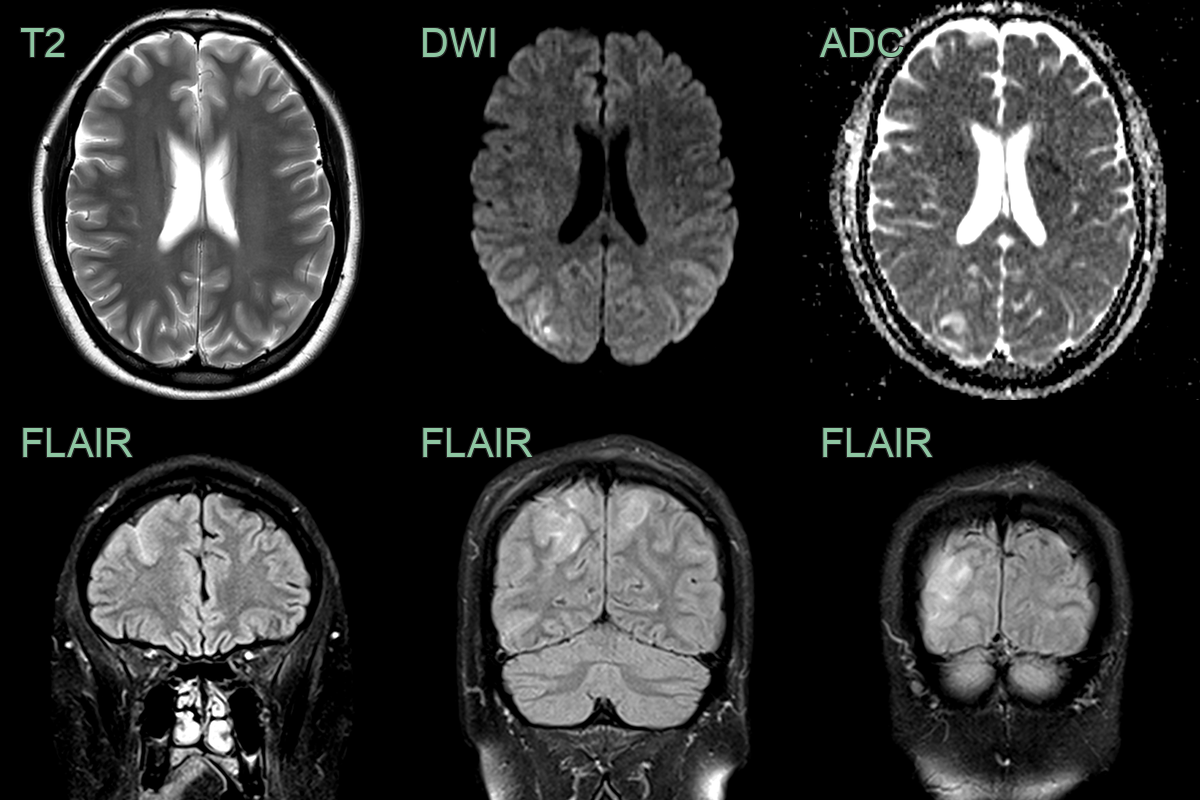
- 25-year-old patient had an emergency c-section for eclampsia.
- MRI was performed after the patient developed an occipital headache, visual disturbance, and vomiting.
- MRI showed cortical and subcortical T2 and FLAIR hyperintensity and a trace of subarachnoid blood.
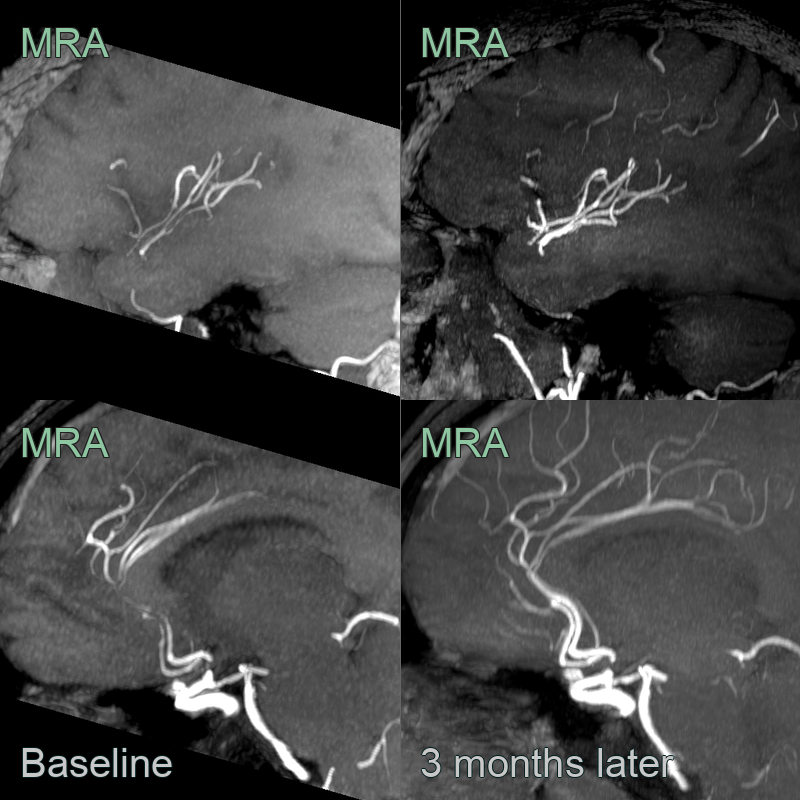
- MRA showed stenoses and irregularity of the A2 ACAs and the right M2 MCAs.
- The findings fully resolved on imaging 3 months later.

- A 40-year-old patient presented with a severe occipital and temporal headache, nausea, vomitting and dizziness.
- MRI showed focal stenoses in the M2 MCAs and both PCAs, which resolved after 6 months.
Treatment¶
- Supportive care and removal of potential triggers
- Calcium channel blockers:
- Nimodipine: first-line treatment (60mg every 4-8 hours for 4-12 weeks)
- Verapamil: alternative option
- Short course of glucocorticoids in severe cases
- Management of complications:
- Anticonvulsants for seizures
- Blood pressure control for hypertension
- Follow-up imaging at 3 months to confirm resolution of vasoconstriction
- Patient education on avoiding triggers and recognising symptoms
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Aneurysmal SAH with vasospasm | Aneurysm visible on CTA/DSA; diffuse basilar subarachnoid blood on CT; vasospasm develops 4-14 days after ictus rather than at headache onset |
| Primary angiitis of CNS (PACNS) | Irreversible arterial narrowing on follow-up MRA; vessel wall enhancement on high-resolution MRI; cortical and subcortical infarcts in multiple vascular territories |
| Posterior reversible encephalopathy syndrome | Posterior-predominant vasogenic oedema on T2/FLAIR; elevated ADC values (not restricted); no multifocal arterial beading on MRA |
| Cerebral venous sinus thrombosis | Filling defects in dural venous sinuses on CT/MR venography; venous infarcts crossing arterial territories; no arterial beading |
| Cervical arterial dissection | Crescentic intramural haematoma on T1 fat-saturated images; eccentric arterial narrowing; may show double lumen |
| Infectious vasculitis (fungal or bacterial meningitis) | Basilar meningeal enhancement; multifocal perforator territory infarcts; stenosis does not resolve on follow-up imaging |