Remote Cerebellar Haemorrhage¶
Summary
- Rare complication following supratentorial or spinal surgery
- Characterised by unexpected cerebellar haemorrhage distant from the operative site
- Typically presents with delayed neurological deterioration post-surgery
Pathophysiology¶
- Exact mechanism remains unclear, but leading theories include:
- Cerebrospinal fluid (CSF) overdrainage leading to downward cerebellar displacement and venous stretching
- Transient increase in intracranial pressure causing venous hypertension
- Intraoperative head positioning causing alterations in venous drainage
Demographics¶
- Incidence: 0.08% to 0.6% of supratentorial craniotomies
- More common in:
- Middle-aged to elderly patients
- Patients with pre-existing coagulopathies
- Cases involving significant CSF drainage during surgery
Diagnosis¶
- Clinical presentation:
- Delayed onset of symptoms (usually 16-72 hours post-surgery)
- Decreased level of consciousness
- Cerebellar signs (ataxia, dysmetria)
- Headache and nausea/vomiting
- Laboratory findings:
- Coagulation profile may reveal abnormalities
- CSF analysis typically normal unless complicated by infection
Imaging¶
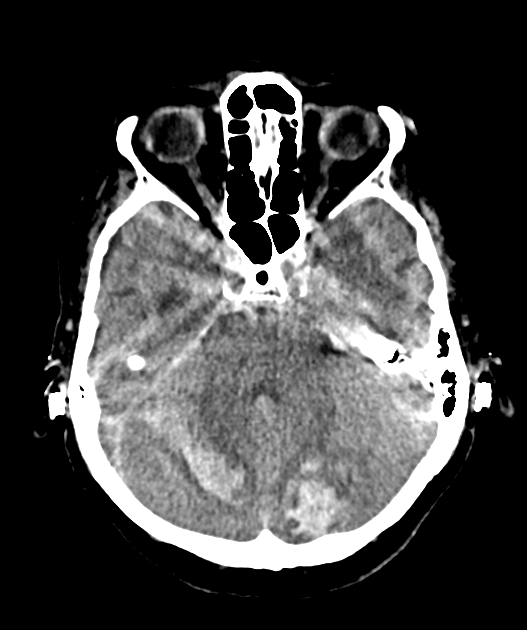
- CT findings:
- Hyperdense cerebellar haemorrhage, often bilateral and symmetrical
- Classic 'zebra sign' or 'streaked bleeding' pattern along cerebellar folia
- May be accompanied by subarachnoid haemorrhage or intraventricular extension
- MRI findings:
- T1: Hyperintense signal in subacute stage
- T2: Mixed signal intensity
- Gradient Echo/SWI: Hypointense blooming artefact confirming haemorrhage
- DWI: May show restricted diffusion in acute stage
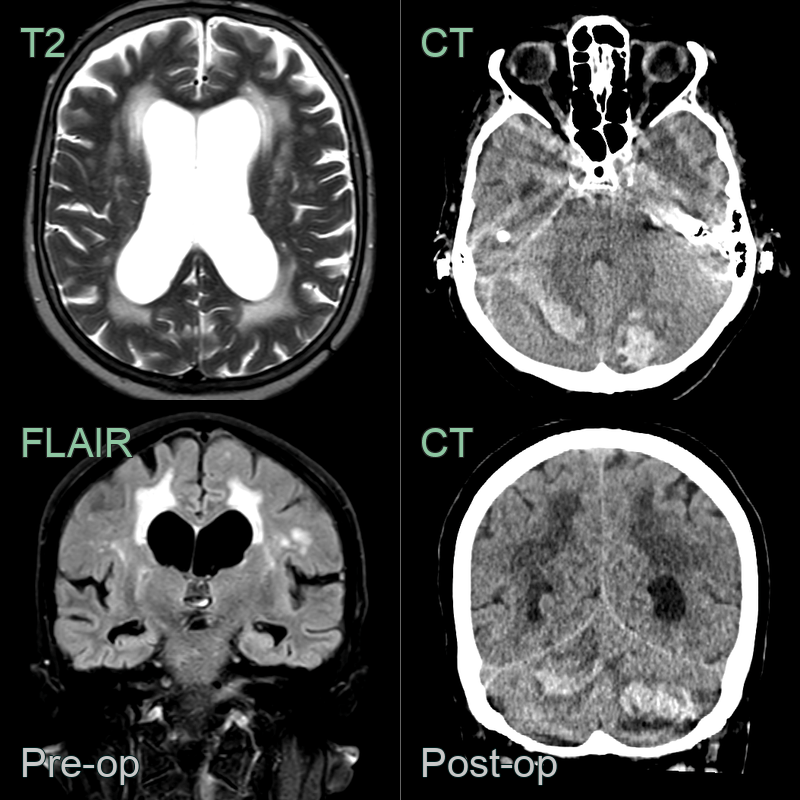
- A 70-year-old patient with ventriculomegaly and a clinical diagnosis of normal pressure hydrocephalus was admitted for the insertion of a ventriculoperitoneal shunt.
- The patient developed cerebellar haemorrhage on the first post-operative day.
Treatment¶
- Management approach depends on severity:
- Conservative management for small haemorrhages:
- Close neurological monitoring
- Blood pressure control
- Reversal of coagulopathy if present
- Surgical intervention for large haemorrhages or significant mass effect:
- Posterior fossa decompression
- Haematoma evacuation
- Conservative management for small haemorrhages:
- Preventive measures:
- Gradual CSF drainage during surgery
- Careful positioning of the head during and after surgery
- Meticulous haemostasis and management of coagulation parameters
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Cerebellar infarction haemorrhagic transformation | Typically follows vascular territory; may have associated brainstem infarcts |
| Cerebellar tumour | Usually more focal; may have mass effect and surrounding oedema |
| Cerebellar abscess | Ring-enhancing lesion with restricted central DWI; surrounding vasogenic oedema |
| Cerebellar metastases | Multiple lesions; ring or nodular enhancement; surrounding vasogenic oedema |
| Cerebellar contusion | Associated overlying scalp/skull injury on CT; localised haemorrhage without supratentorial craniotomy site |
| Cerebellar arteriovenous malformation | Serpiginous vascular structures; flow voids on MRI |
| Cerebellar venous thrombosis | Venous infarction; may see thrombosed veins on imaging |