Sarcoidosis¶
Summary
- Multisystem granulomatous disorder of unknown aetiology
- Characterised by non-caseating granulomas in affected organs
- Primarily affects lungs and lymph nodes; can involve any organ system
Pathophysiology¶
- Exact cause unknown; likely involves abnormal immune response to environmental triggers
- Formation of non-caseating granulomas in affected tissues
- Granulomas consist of epithelioid cells, multinucleated giant cells, and lymphocytes
- Activated T-cells and macrophages play a key role in granuloma formation
Demographics¶
- Peak incidence: 20-40 years of age
- More common in women
- Higher prevalence in African Americans and Northern Europeans
- Familial clustering suggests genetic predisposition
Diagnosis¶
- No single diagnostic test; based on clinical presentation, imaging, and histopathology
- Exclusion of other granulomatous diseases (e.g., tuberculosis, fungal infections)
- Elevated serum angiotensin-converting enzyme (ACE) levels in 60-80% of cases
- Bronchoalveolar lavage: increased CD4/CD8 T-cell ratio
- Tissue biopsy: non-caseating granulomas
Imaging¶
-
Chest radiography:
- Bilateral hilar lymphadenopathy (most common finding)
- Reticular opacities and nodules in lung parenchyma
- Staging system based on chest X-ray findings (Scadding stages 0-IV)
-
High-resolution CT (HRCT):
- Perilymphatic nodules
- Ground-glass opacities
- Fibrotic changes in advanced stages
- Mediastinal and hilar lymphadenopathy
-
18F-FDG PET/CT:
- Useful for assessing disease activity and extrapulmonary involvement
- Increased FDG uptake in active granulomatous lesions
-
Cardiac MRI:
- Evaluation of cardiac sarcoidosis
- Late gadolinium enhancement in affected myocardium
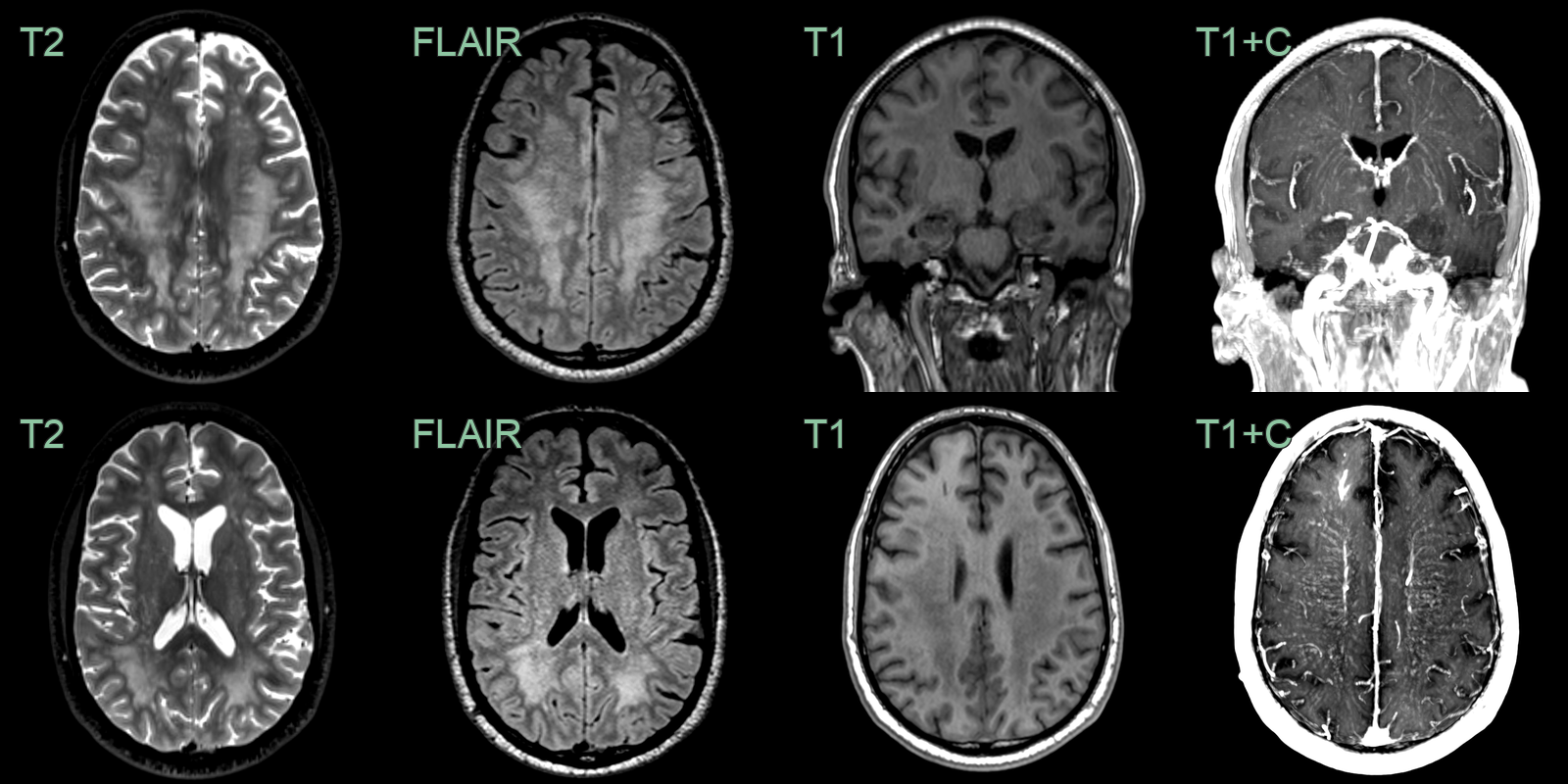
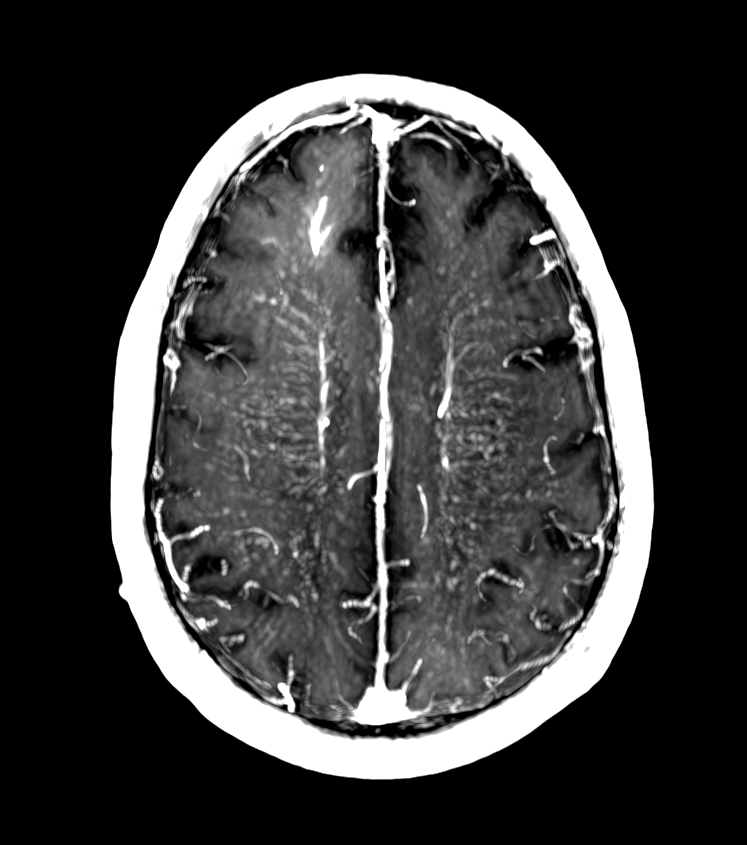
- A 50-year-old patient presented with vague neurological symptoms including cognitive impairment.
- MRI showed a diffuse leukoencephalopathy with striking perivascular enhancement.
- Biopsy revealed granulomatous inflammation compatible with neurosarcoidosis.
Treatment¶
- Many patients require no treatment; spontaneous remission in up to 60% of cases
-
Corticosteroids: first-line therapy for symptomatic or progressive disease
- Prednisone: initial dose 20-40 mg/day, tapered over 6-12 months
-
Second-line agents for refractory cases or steroid-sparing:
- Methotrexate
- Azathioprine
- Hydroxychloroquine
- Anti-TNF-α agents (e.g., infliximab)
-
Organ-specific treatments:
- Cardiac sarcoidosis: antiarrhythmic drugs, implantable cardioverter-defibrillators
- Ocular sarcoidosis: topical corticosteroids, immunosuppressants
-
Regular follow-up and monitoring of organ function and treatment response
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Lymphoma (primary CNS or systemic) | Periventricular mass lesions with ring or homogeneous enhancement; marked diffusion restriction on DWI; no perivascular predilection |
| Tuberculosis | Predominantly basilar leptomeningeal enhancement; ring-enhancing tuberculomas with central restricted diffusion; calcifications on CT |
| IgG4-related disease | Nodular dural/pachymeningeal thickening and enhancement; orbital pseudotumour; pituitary stalk and infundibular involvement |
| Leptomeningeal carcinomatosis | Diffuse nodular leptomeningeal enhancement without perivascular predominance; may involve cranial nerves diffusely |
| Multiple sclerosis | Periventricular ovoid white matter lesions (Dawson's fingers); calloso-septal interface lesions; no leptomeningeal or cranial nerve enhancement |
| Langerhans cell histiocytosis | Hypothalamic and pituitary stalk thickening; lytic skull lesions on CT; absence of perivascular leptomeningeal enhancement |
| Neurosyphilis | Meningeal enhancement and vessel wall involvement on high-resolution MRI; can appear identical to neurosarcoidosis |
| Granulomatosis with polyangiitis (GPA) | Skull base destruction and paranasal sinus involvement on CT; orbital soft tissue infiltration; dural-based enhancing masses |