Secondary CNS Lymphoma¶
Summary
- Secondary CNS lymphoma (SCNSL) refers to CNS involvement in patients with systemic lymphoma
- Typically occurs in advanced stages of systemic disease or at relapse
- Imaging findings include single or multiple enhancing lesions, often with periventricular distribution
Pathophysiology¶
- Results from hematogenous spread or direct extension from adjacent structures
- Most commonly associated with aggressive B-cell non-Hodgkin lymphomas, particularly diffuse large B-cell lymphoma (DLBCL)
- Disruption of blood-brain barrier facilitates lymphoma cell entry into CNS
Demographics¶
- Incidence: 5-10% of patients with systemic lymphoma
- Risk factors:
- High-grade lymphomas
- Advanced stage disease
- Extranodal involvement
- Elevated serum LDH levels
- Median age at diagnosis: 60-65 years
- Slight male predominance
Diagnosis¶
- Clinical presentation:
- Neurological deficits (e.g., focal weakness, sensory changes)
- Cognitive impairment
- Headache
- Seizures
- Diagnostic workup:
- Neuroimaging (MRI with contrast)
- CSF analysis (cytology, flow cytometry, immunoglobulin gene rearrangement)
- Brain biopsy (if diagnosis remains uncertain)
Imaging¶
- MRI findings:
- Single or multiple enhancing lesions
- Periventricular distribution common
- T1: hypointense to isointense
- T2/FLAIR: hyperintense
- Diffusion restriction often present
- Contrast enhancement: homogeneous or ring-like
- CT findings:
- Hyperdense lesions
- Contrast enhancement
- Differential diagnosis:
- Metastases
- Primary CNS lymphoma
- Infectious processes (e.g., toxoplasmosis, tuberculoma)
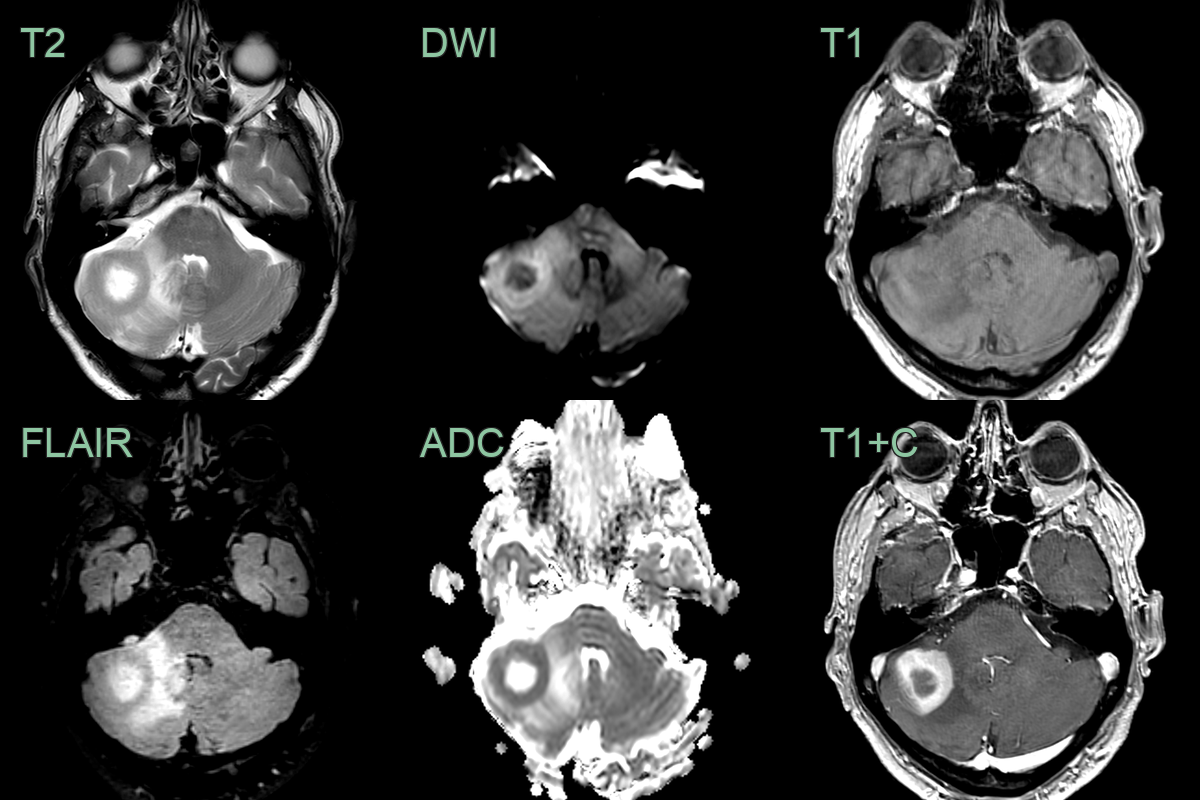
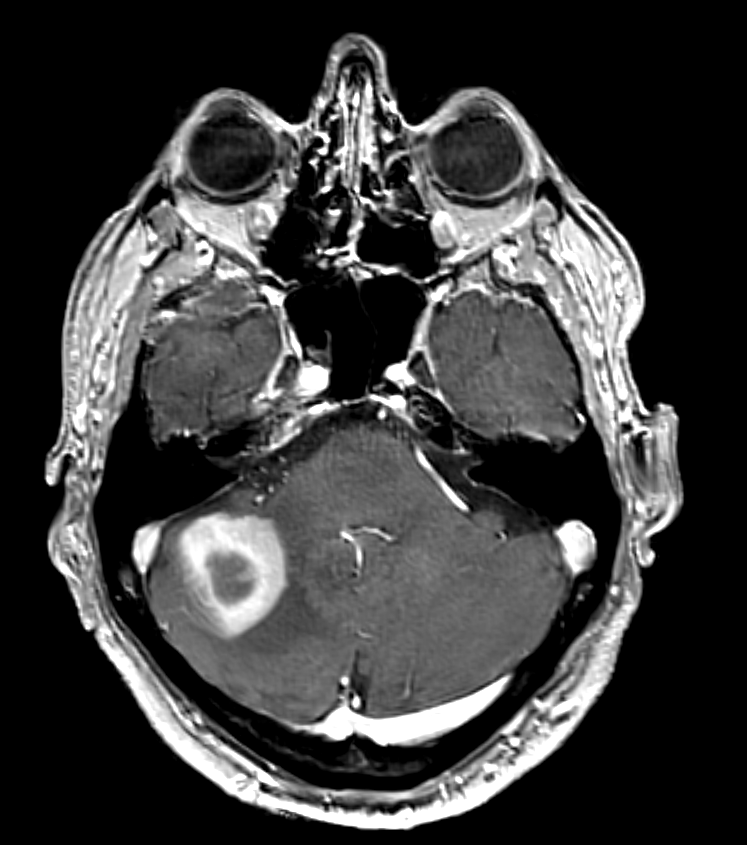
- An 80-year old who underwent systemic treatment for a systemic high-grade B cell lymphoma.
- 6 months later, the patient present with worsening ataxia.
- MRI showed a right cerebellar lesion with a thick band of peripheral enhancement and diffusion restriction.
- Biopsy confirmed a CNS relapse of a B cell lymphoma.
Treatment¶
- Systemic therapy:
- High-dose methotrexate-based regimens
- Rituximab for CD20-positive lymphomas
- CNS-directed therapy:
- Intrathecal chemotherapy
- Whole-brain radiotherapy (WBRT) for extensive disease or palliation
- Supportive care:
- Corticosteroids for cerebral oedema
- Anticonvulsants for seizure control
- Prognosis:
- Generally poor, with median survival of 2-6 months without treatment
- Improved outcomes with aggressive multimodal therapy
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Primary CNS Lymphoma | Imaging-identical appearance; periventricular homogeneously enhancing mass with marked diffusion restriction |
| Metastatic Brain Tumour | Often multiple lesions at grey-white matter junction; ring or nodular enhancement; surrounding vasogenic oedema |
| Glioblastoma | Typically single lesion; heterogeneous ring enhancement with central necrosis; infiltrative margins on T2/FLAIR |
| Multiple Sclerosis | Ovoid periventricular lesions; incomplete ring or no enhancement; no mass effect |
| Cerebral Abscess | Ring-enhancing lesion with restricted diffusion in the cavity and elevated signal on DWI; thin smooth enhancing wall |
| Toxoplasmosis | Multiple ring-enhancing lesions in basal ganglia and at grey-white matter junction; restricted diffusion in centre |
| Progressive Multifocal Leukoencephalopathy | Non-enhancing asymmetric subcortical white matter lesions with scalloped margins; no mass effect |
| Acute Disseminated Encephalomyelitis | Bilateral, often large confluent white matter lesions involving grey matter; incomplete ring enhancement |
| Neurosarcoidosis | Leptomeningeal and perivascular enhancement; cranial nerve involvement; hilar lymphadenopathy on chest CT |
| CNS Vasculitis | Multifocal infarcts in multiple vascular territories; vessel wall enhancement on high-resolution MRI |