Silent Sinus Syndrome¶
Summary
- Chronic maxillary sinus atelectasis causing enophthalmos and facial asymmetry
- Characterised by painless, spontaneous collapse of the maxillary sinus
- Diagnosis based on clinical presentation and distinctive imaging findings
Pathophysiology¶
- Chronic hypoventilation of the maxillary sinus due to ostial obstruction
- Negative pressure within the sinus leads to:
- Resorption of sinus contents
- Inward bowing of sinus walls
- Downward displacement of the orbital floor
- Exact etiology remains unclear, but may involve:
- Congenital anatomical variations
- Chronic sinusitis
- Previous sinus surgery
Demographics¶
- Typically affects adults in their 3rd to 5th decades of life
- No gender predilection
- Rare condition, with limited epidemiological data available
Diagnosis¶
- Clinical presentation:
- Painless, gradual enophthalmos
- Facial asymmetry
- Deepening of the superior sulcus
- Hypoglobus
- Often asymptomatic or minimally symptomatic
- Absence of significant sinonasal symptoms
Imaging¶
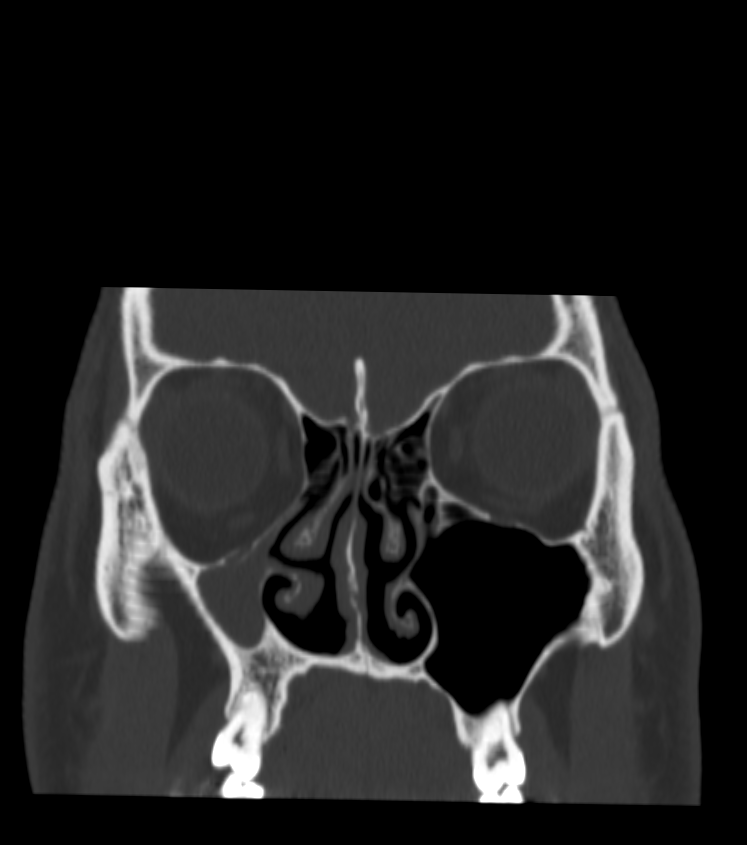
- CT scan is the gold standard for diagnosis
- Unilateral opacification and volume loss of the maxillary sinus
- Inward bowing of sinus walls (lateral, superior, and medial)
- Downward displacement of the orbital floor
- Widening of the middle meatus
- Lateralization of the uncinate process
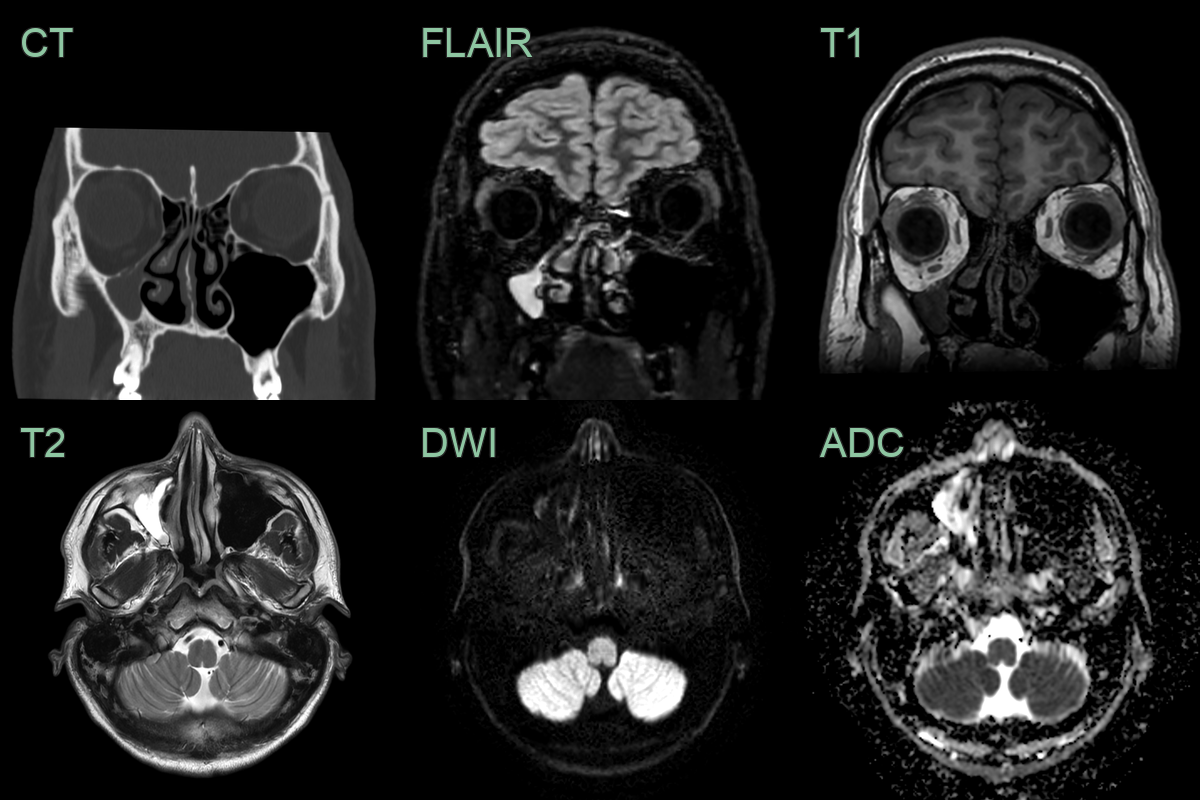
- MRI:
- May show T2 hypointensity within the affected sinus
- Useful for evaluating orbital soft tissues
- An incidental finding was a small volume fluid filled maxillary sinus.
- The walls of the maxillary sinus were normally formed with no evidence of prior trauma.
- The floor of the orbit was depressed, with compenstatory enlargement of the orbit.
- There was a hypoglobus of 2 mm.
Treatment¶
- Surgical management is the primary treatment
- Endoscopic sinus surgery:
- Maxillary antrostomy to restore sinus ventilation
- Uncinectomy and ethmoidectomy as needed
- Orbital floor reconstruction:
- May be performed simultaneously or as a staged procedure
- Indicated for significant enophthalmos or hypoglobus
- Materials for orbital floor reconstruction:
- Autologous bone grafts
- Alloplastic implants (e.g., titanium mesh, porous polyethylene)
- Post-operative follow-up:
- Monitor for resolution of sinus opacification
- Assess improvement in facial symmetry and orbital position
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Chronic sinusitis | Thickened sinus mucosa with air-fluid level; sinus volume normal; no progressive reduction in sinus volume or enophthalmos |
| Orbital floor fracture | Visible fracture line on CT; associated soft tissue herniation or entrapment; no reduction in sinus volume |
| Granulomatosis with polyangiitis (GPA) | Destructive sinonasal lesions with bone destruction; soft tissue masses in sinuses; septal perforation |
| Orbital tumour | Solid mass within the orbit causing proptosis rather than enophthalmos; no sinus collapse |
| Osteomyelitis | Bone destruction with periosteal reaction and soft tissue swelling; no inward retraction of sinus walls |
| Mucocele | Expansile lesion with outward bowing of sinus walls; often associated with proptosis rather than enophthalmos |
| Fibrous dysplasia | Ground-glass appearance of bone on CT; expanded rather than contracted sinus; typically involves multiple bones |
| Metastatic disease | Multiple lytic lesions throughout skull base and facial bones; no pattern of sinus contraction |