Stroke-like Migraine Attacks after Radiation Therapy (SMART)¶
Summary
- SMART syndrome is a rare delayed complication of cranial irradiation
- Characterised by recurrent, reversible neurological deficits and headaches
- Distinctive imaging findings include cortical enhancement and oedema
Pathophysiology¶
- Exact mechanism remains unclear, but proposed theories include:
- Endothelial dysfunction and blood-brain barrier disruption
- Neuronal excitotoxicity and cortical spreading depression
- Radiation-induced vascular damage and altered neurovascular coupling
Demographics¶
- Typically occurs in patients who have received cranial irradiation for primary or metastatic brain tumours
- Median time to onset: 20 years post-radiation (range: 1-37 years)
- No clear gender predilection
- Most commonly affects adults, but cases in children have been reported
Diagnosis¶
- Clinical presentation:
- Acute onset of neurological deficits (e.g., hemiparesis, aphasia, visual disturbances)
- Severe headache, often migraine-like
- Seizures in some cases
- Diagnostic criteria proposed by Black et al. (2006) :
- Remote history of cranial irradiation
- Prolonged, reversible neurological deficit
- Cortical gadolinium enhancement on MRI
- Eventual complete or partial recovery
Imaging¶
- MRI findings:
- Unilateral or bilateral cortical enhancement, typically gyriform pattern
- Cortical swelling and oedema in the affected region
- Restricted diffusion may be present
- Perfusion imaging may show hyperperfusion
- CT findings:
- Often normal or may show subtle hypodensity in the affected cortex
- Follow-up imaging:
- Resolution of enhancement and oedema over weeks to months
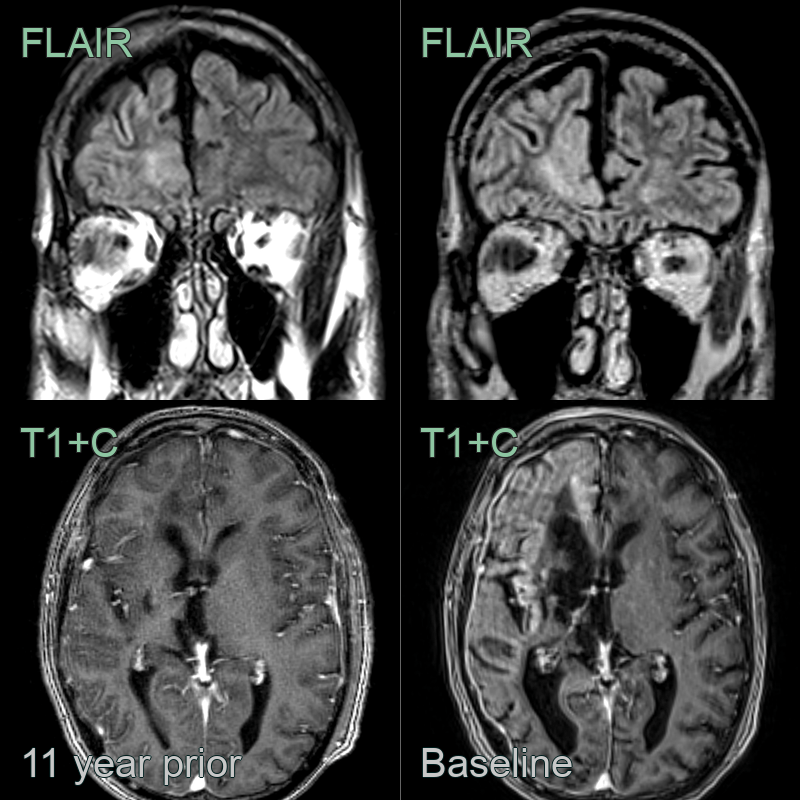
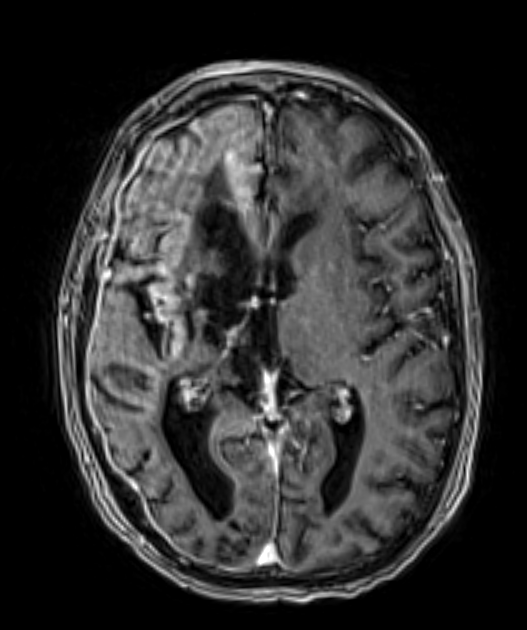
- 50-year-old patient with a history of primary CNS lymphoma 20 years ago that was treated with cranial irradiation.
- The patient presented with headache, confusion and left sided weakness.
- MRI showed subtle increase in T2-weighted hyperintensity in the right forntal cortex and gyriform enhancement.
- CSF analysis did not show any evidence of disease recurrence and imaging 1 year later showed partial resolution of the gyral enhancement.
Treatment¶
- Supportive care is the mainstay of treatment
- Symptomatic management:
- Analgesics for headache
- Anticonvulsants if seizures are present
- Corticosteroids may be beneficial in some cases
- Prophylactic treatments reported with variable success:
- Verapamil
- Aspirin
- Topiramate
- Patient education about the typically self-limiting nature of episodes
- Long-term follow-up to monitor for recurrence and exclude tumour progression
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Stroke / infarction | Persistent DWI restriction confined to an arterial vascular territory; no resolution on follow-up; no associated gyral enhancement |
| Radiation necrosis | Progressive enhancing mass with surrounding oedema and mass effect; elevated choline on MR spectroscopy; no spontaneous resolution |
| Tumour recurrence | Progressive enhancing lesion with elevated rCBV and choline on advanced MRI; no spontaneous resolution |
| Posterior reversible encephalopathy syndrome (PRES) | Posterior-predominant bilateral vasogenic oedema on T2/FLAIR; elevated ADC; no gyral enhancement in the radiation field |
| Encephalitis | Mesiotemporal or bilateral cortical T2/FLAIR hyperintensity with DWI restriction; enhancement; not confined to radiation field |
| Seizure-related cortical changes (Todd's) | Transient cortical FLAIR hyperintensity and swelling; resolves rapidly; DWI changes limited to cortex |