Solitary Fibrous Tumour¶
Summary
- Rare mesenchymal neoplasm of fibroblastic origin
- Can occur in various anatomical locations, most commonly pleura
- Typically presents as a slow-growing, well-circumscribed mass with variable imaging features
Pathophysiology¶
- Derived from CD34-positive fibroblastic cells
- Characterised by NAB2-STAT6 gene fusion, resulting in STAT6 nuclear expression
- Majority are benign, but 10-20% may show malignant behaviour
Demographics¶
- Can occur at any age, peak incidence in the 5th-6th decades
- No significant gender predilection
- Most common in pleura, but can occur in various extrapleural sites (e.g., meninges, orbit, soft tissues)
Diagnosis¶
- Often asymptomatic, discovered incidentally
- Symptoms depend on location and size:
- Pleural: dyspnea, chest pain
- CNS: headache, seizures, focal neurological deficits
- Soft tissue: painless mass
- Diagnosis confirmed by histopathology and immunohistochemistry (CD34, STAT6 positive)
Imaging¶
- CT:
- Well-circumscribed, lobulated mass
- Heterogeneous enhancement
- Calcifications in 10% of cases
- MRI:
- T1: isointense to muscle
- T2: variable, often heterogeneous with areas of high and low signal intensity
- Strong enhancement after gadolinium administration
- "Flow voids" may be present due to prominent vessels
- Angiography:
- Hypervascular lesion with prominent feeding vessels
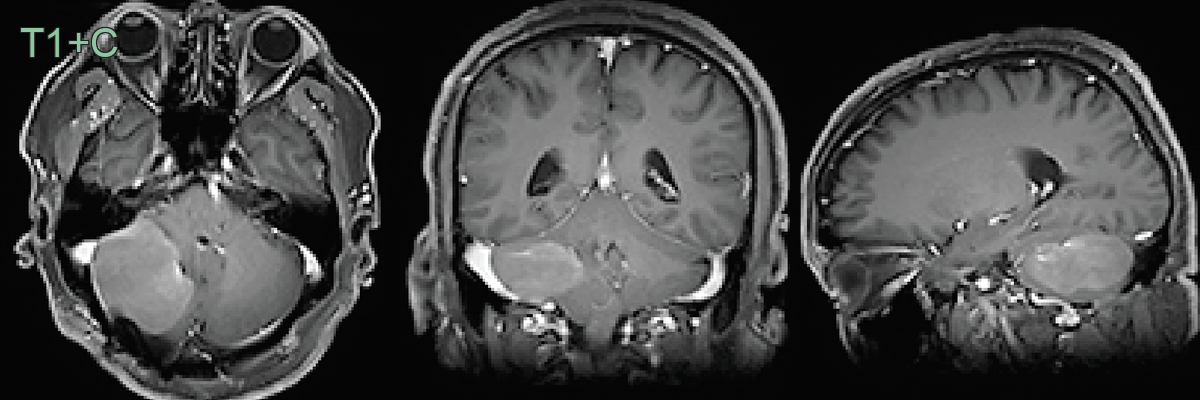
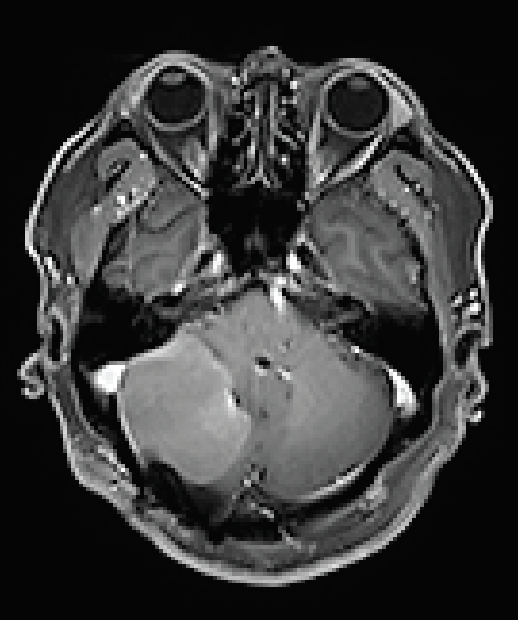
- 63-year-old patient presentd with walking instability.
- MRI showed an enhancing well-defined extra-axial lesion distorting the right cerebellar hemisphere.
- Imaging modified from Zhu et al1.
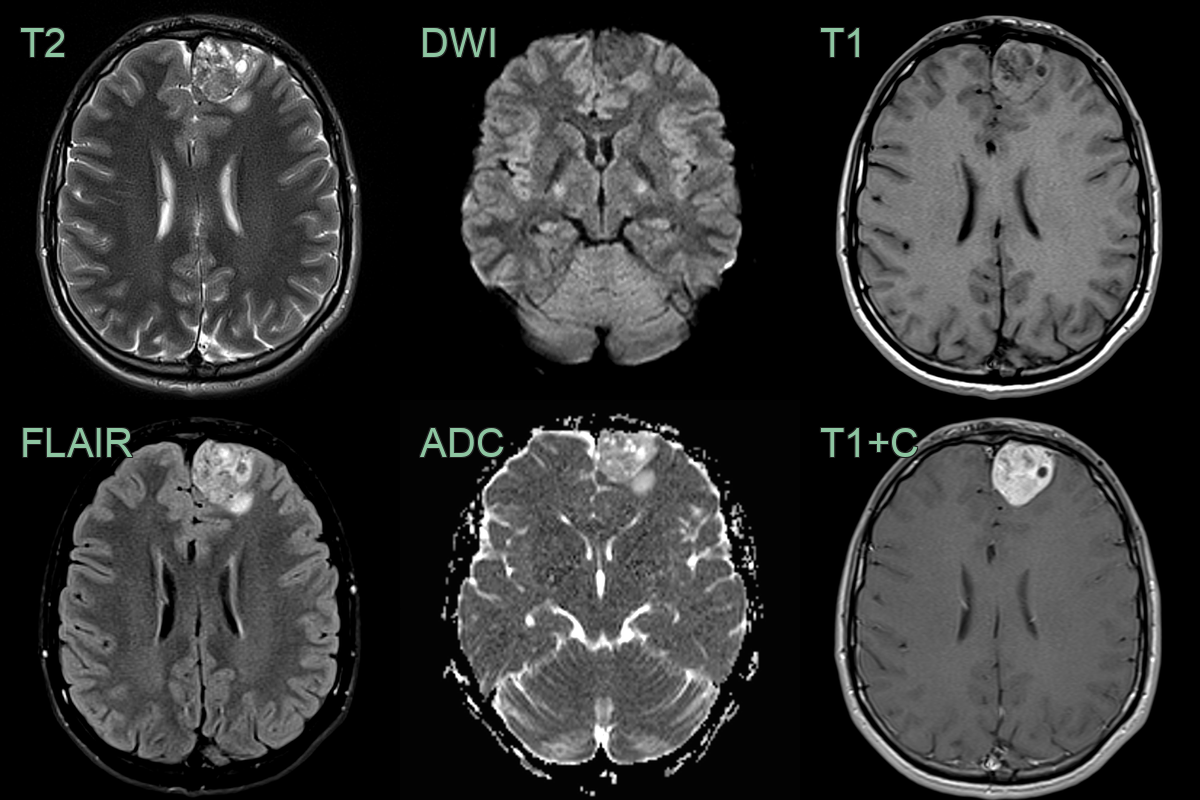
- A 30-year-old patient presented following a seizure.
- MRI showed a heterogeneously T2-hyperintense and enhancing lesion over the left frontal pole.
- The lesion was resected and a solitary fibrous tumour was diagnosed.
Treatment¶
- Surgical resection is the primary treatment modality
- Complete resection associated with better prognosis
- Adjuvant radiotherapy may be considered for incompletely resected tumours
- Chemotherapy reserved for metastatic or unresectable disease
- Long-term follow-up recommended due to risk of late recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Meningioma | Dural tail sign on contrast MRI; may calcify; more commonly convexity-based |
| Schwannoma | Eccentric growth along cranial nerve; cystic degeneration common; no "yin-yang" T2 pattern |
| Hemangioblastoma | Large cyst with small enhancing mural nodule; no lobulated solid mass; associated with VHL |
| Metastatic tumour | Often multiple extra-axial or intraparenchymal lesions; surrounding vasogenic oedema |
| Glioblastoma | Infiltrative intraparenchymal mass with ring enhancement and central necrosis; not extra-axial |
References¶
-
Zhu et al. Malignant Solitary Fibrous Tumor of the Right Cerebellum: A Case Report. 2021. Case Reports in Neurology - Open in new tab. ↩