Spinal Chondrosarcoma¶
Summary

- Rare malignant cartilaginous tumour of the spine
- Typically presents with pain, neurological deficits, and palpable mass
- Imaging shows lytic lesion with calcifications and soft tissue extension
Pathophysiology¶
- Arises from cartilage-forming cells in the spine
- Can be primary or secondary (arising from pre-existing benign cartilaginous lesion)
- Graded I-III based on cellularity, nuclear atypia, and mitotic activity
- Most common in the thoracic spine, followed by cervical and lumbar regions
Demographics¶
- Accounts for approximately 10% of all chondrosarcomas
- Peak incidence in 4th to 6th decades of life
- Slight male predominance (1.5:1 male to female ratio)
- No known ethnic predisposition
Diagnosis¶
- Clinical presentation:
- Localised pain (often worse at night)
- Neurological deficits due to spinal cord or nerve root compression
- Palpable mass in some cases
- Histopathology:
- Biopsy required for definitive diagnosis
- Shows malignant chondrocytes with varying degrees of differentiation
- Immunohistochemistry positive for S-100 protein
Imaging¶
- Plain radiographs:
- Lytic lesion with endosteal scalloping
- Calcifications within the tumour matrix (ring and arc pattern)
- CT:
- Better delineation of calcifications and cortical destruction
- Useful for surgical planning
- MRI:
- T1: Low to intermediate signal intensity
- T2: High signal intensity with low signal foci (calcifications)
- Contrast enhancement: Heterogeneous enhancement
- Useful for assessing soft tissue extension and spinal cord compression
- Bone scintigraphy:
- Increased uptake in the lesion
- Useful for detecting metastases
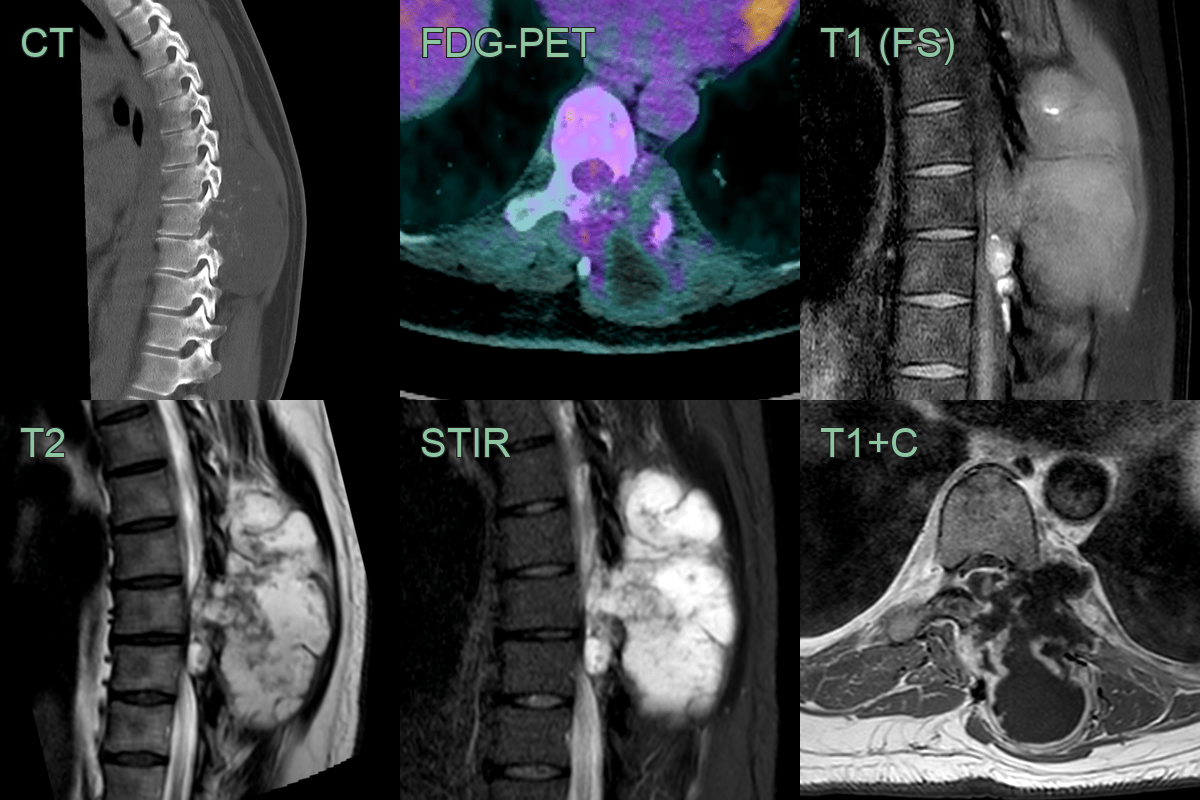
- 35-year-old patient presented with back pain.
- CT showed a descructive midthoracic lesion.
- MRI showed a lobulated T2-hyperintense and peripherally enhancing lesion with a small intraspinal component.
- The enhancing components of the lesion where avid on FDG-PET.
Treatment¶
- Surgical resection:
- En bloc resection with wide margins is the gold standard
- Challenging due to proximity to vital structures
- Adjuvant therapy:
- Radiation therapy for incompletely resected tumours or high-grade lesions
- Limited role of chemotherapy, mainly used for metastatic disease
- Prognosis:
- 5-year survival rates vary based on grade:
- Grade I: 90%
- Grade II: 60-70%
- Grade III: 30-40%
- Follow-up:
- Regular imaging surveillance for local recurrence and metastases
- Long-term follow-up required due to risk of late recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Chordoma | Typically midline location; arises from notochord remnants |
| Osteosarcoma | More aggressive bone destruction; periosteal reaction |
| Giant Cell Tumour | Eccentric location; geographic lytic lesion with sharp margins; no chondroid matrix or calcifications |
| Metastatic Disease | Multiple lesions; more aggressive bone destruction; no chondroid matrix |
| Ewing Sarcoma | Permeative pattern with onion-skin periosteal reaction; large disproportionate soft tissue mass; no chondroid calcifications |
| Osteochondroma | Continuous with underlying bone cortex and medullary cavity; cartilaginous cap of normal thickness |
| Enchondroma | Usually smaller and intramedullary; lacks soft tissue component; no bone destruction |
| Aneurysmal Bone Cyst | Multiple fluid-fluid levels on MRI; expansile with thin cortical shell; no solid enhancing matrix |
| Hemangioma | Characteristic trabecular "corduroy" pattern on CT; high T1 and T2 signal on MRI |
| Lymphoma | Permeative marrow infiltration with relative cortical preservation; no chondroid matrix or calcifications |