Spinal Cord Infarct¶
Summary

- Acute onset of neurological deficits due to ischaemia of the spinal cord
- Presents with sudden weakness, sensory loss, and autonomic dysfunction
- Diagnosis relies on clinical presentation and MRI findings
Pathophysiology¶
- Caused by interruption of blood supply to the spinal cord, leading to tissue ischaemia and necrosis
- Common aetiologies:
- Atherosclerosis of spinal arteries
- Embolic events
- Aortic dissection or surgery
- Vasculitis
- Hypotension or hypoperfusion states
Demographics¶
- Rare condition, accounting for 1-2% of all strokes
- More common in older adults (>60 years)
- Slight male predominance
- Risk factors:
- Hypertension
- Diabetes mellitus
- Smoking
- Hyperlipidaemia
Diagnosis¶
- Clinical presentation:
- Sudden onset of neurological deficits
- Bilateral weakness or paralysis
- Sensory loss below the level of infarction
- Autonomic dysfunction (e.g., urinary retention, bowel incontinence)
- Differential diagnosis:
- Transverse myelitis
- Spinal cord compression
- Guillain-Barré syndrome
- Laboratory tests:
- CSF analysis to rule out infectious causes
- Serum inflammatory markers
Imaging¶
- MRI is the gold standard for diagnosis
- T2-weighted and STIR sequences:
- Hyperintense signal within the spinal cord
- "Owl's eyes" appearance in axial views (central grey matter involvement)
- Diffusion-weighted imaging (DWI):
- Restricted diffusion in acute phase
- Contrast-enhanced T1-weighted:
- Minimal or no enhancement in acute phase
- CT angiography:
- Useful for identifying vascular abnormalities or aortic dissection
- Spinal angiography:
- May be considered in select cases to identify vascular malformations
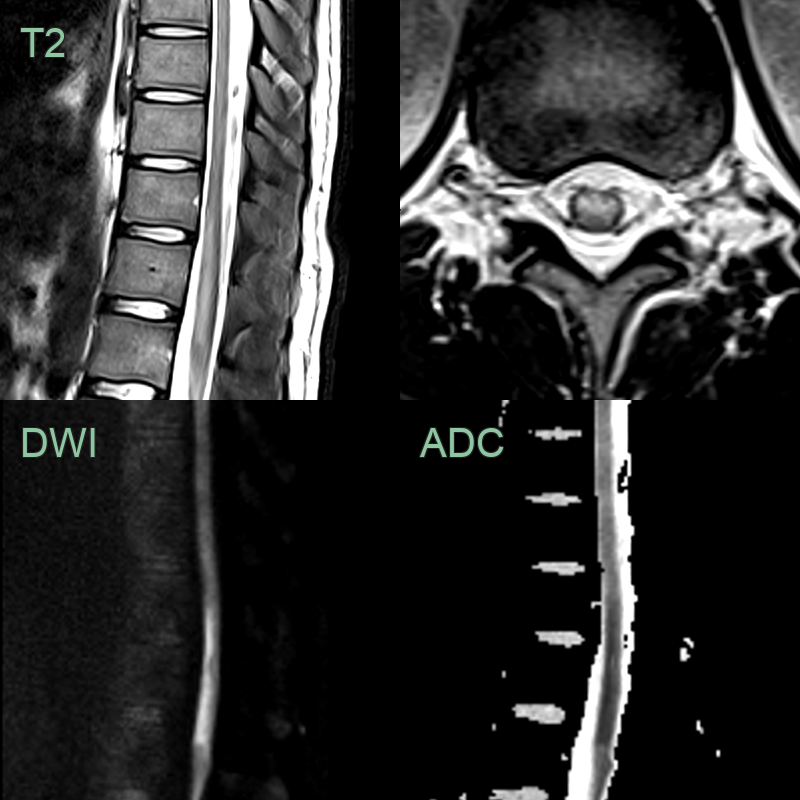
- 40-year-old patient with a cardiac myopathy presented with sudden onset lower back pain and lower limb weakness.
- MRI showed an anterior lower thoracic cord lesion causing diffusion restriction representing an anterior spinal artery infarct.
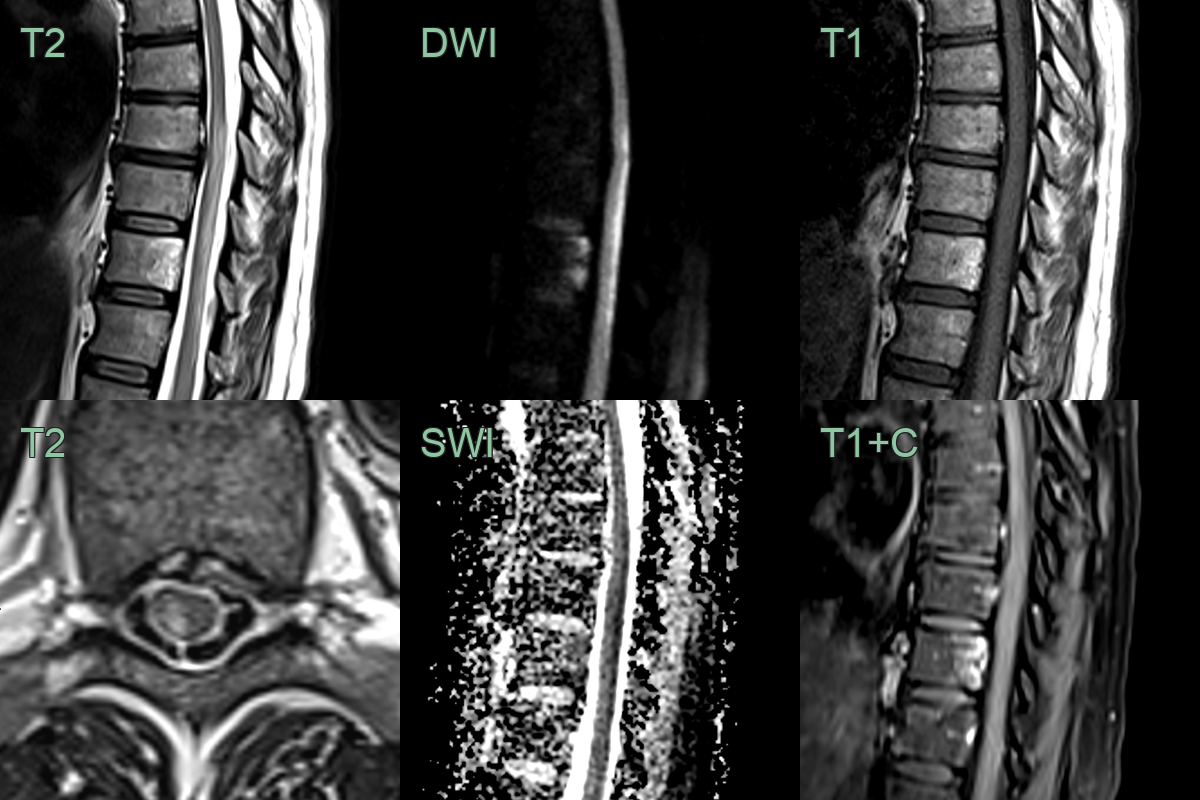
- A 50-year-old patient presented with sudden onset lower limb weakness and sensory disturbance.
- MRI showed a longitudinally extensive dorsal cord lesion (right paramedian) lesion with diffusion restriction.
- There was signal change and enhancement within the dorsal aspect of the T10 vertebral body.
- Appearances are consistent with an infarct in the territory of a right posterior spinal artery.
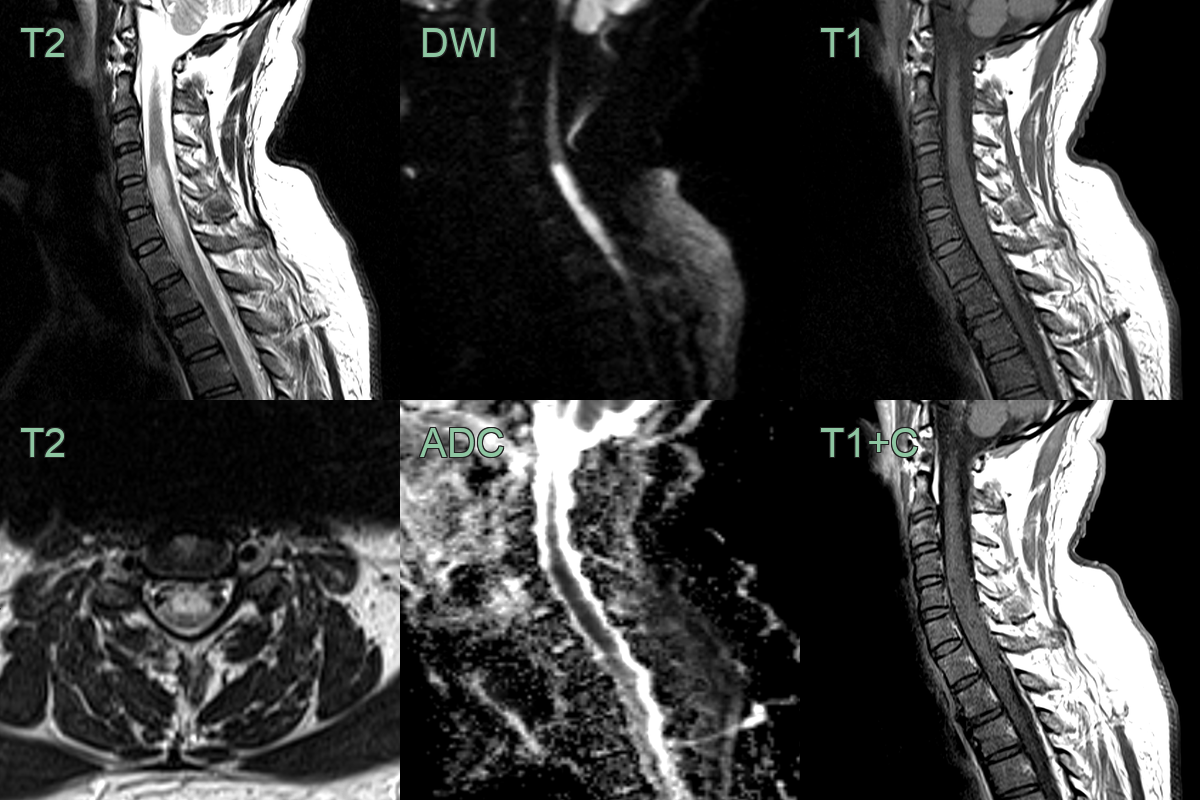
- A 50-year-old patient presented with acute upper back pain and quadriparesis.
- MRI showed a long segment lesion with diffusion restriction without contrast enhancement.
- The involvement of the anterior half of the cord was typical of an acute cord infarct in the territory of the anterior spinal artery.
Treatment¶
- Acute management:
- Maintain adequate spinal cord perfusion
- Blood pressure control
- Antiplatelet therapy (e.g., aspirin)
- Supportive care:
- Respiratory support if needed
- Bladder and bowel management
- Prevention of pressure ulcers
- Rehabilitation:
- Physical therapy
- Occupational therapy
- Speech therapy (if cervical cord involvement)
- Secondary prevention:
- Risk factor modification
- Anticoagulation in select cases (e.g., cardioembolic source)
- Prognosis:
- Variable, depending on the extent and location of infarction
- Complete recovery in 10-20% of cases
- Residual deficits common in severe cases
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Transverse myelitis | Central cord T2 signal without anterior horn predilection; cord swelling and enhancement; may extend over multiple vertebral segments without DWI restriction |
| Multiple Sclerosis | Short cord lesion (<2 vertebral segments); dorsolateral location; multiple periventricular and juxtacortical brain lesions; no restricted diffusion |
| Compressive myelopathy | MRI shows structural compression from disc, osteophyte, or mass; deformity of cord contour; no restricted diffusion acutely |
| Spinal epidural abscess | Rim-enhancing epidural collection displacing the thecal sac; restricted diffusion in the abscess cavity; cord oedema secondary to compression |
| Spinal cord tumour | Intramedullary expansile mass with cord enlargement; heterogeneous enhancement; no restricted diffusion |
| Acute Disseminated Encephalomyelitis | Bilateral white matter T2 lesions in brain and spinal cord; no cord restricted diffusion; no owl-eye or pencil-like DWI pattern |