Spinal Cord Lipoma¶
Summary

- Congenital malformation characterised by abnormal fatty tissue within the spinal cord
- Often associated with spinal dysraphism and tethered cord syndrome
- Imaging crucial for diagnosis, with MRI being the modality of choice
Pathophysiology¶
- Abnormal embryological development of the neural tube and surrounding mesenchymal tissue
- Lipomatous tissue infiltrates the spinal cord, causing mass effect and potential neurological deficits
- Often associated with:
- Spinal dysraphism
- Tethered cord syndrome
- Syringomyelia
Demographics¶
- Incidence: 1 in 4,000 live births
- No significant gender predilection
- Most commonly diagnosed in infancy or early childhood
- Can be detected prenatally with advanced imaging techniques
Diagnosis¶
- Clinical presentation:
- Asymptomatic in some cases
- Cutaneous stigmata (e.g., dimples, hairy patches, subcutaneous masses)
- Neurological deficits (motor, sensory, or sphincter dysfunction)
- Back pain
- Physical examination:
- Neurological assessment
- Inspection of the back for cutaneous markers
- Imaging studies essential for definitive diagnosis
Imaging¶
- Magnetic Resonance Imaging (MRI):
- Gold standard for diagnosis and surgical planning
- T1-weighted images: Hyperintense signal of fatty tissue
- T2-weighted images: Variable signal intensity
- Fat-suppression sequences: Confirm lipomatous nature
- Computed Tomography (CT):
- May show low-density fatty tissue
- Less useful than MRI for soft tissue characterisation
- Ultrasound:
- Useful in neonates and infants with open spinal dysraphism
- Limited utility in older children and adults
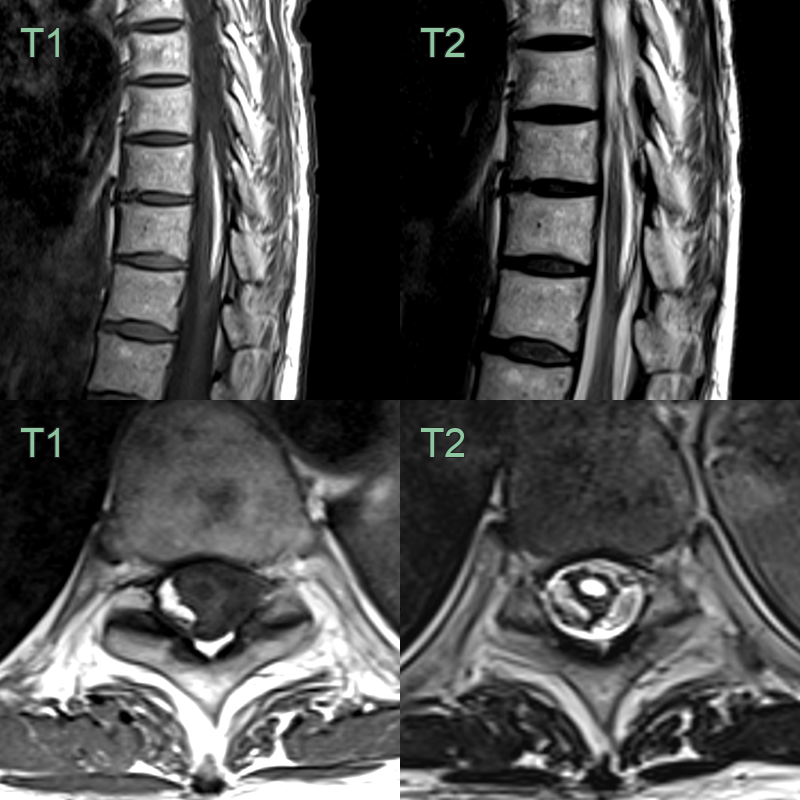
- A 50-year-old patient presented with a radiculopathy caused by lumbar spondylosis.
- Incidentally, the distal cord was expanded by a fat-containing lesion and was associated with a dilated central canal.
Treatment¶
- Conservative management:
- For asymptomatic patients or those with minimal symptoms
- Regular clinical and radiological follow-up
- Surgical intervention:
- Primary goal: Untether the spinal cord and decompress neural elements
- Debulking or resection of lipoma to avoid neurological injury
- Long-term follow-up essential due to risk of re-tethering and progressive neurological deficits
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Spinal cord tumour | Lipomas show fat signal on MRI, while other tumours typically do not |
| Tethered cord syndrome | Lipomas may cause tethering, but not all tethered cords have lipomas |
| Myelomeningocele | Lipomas are intradural, while myelomeningoceles are open neural tube defects |
| Dermoid cyst | Dermoids have heterogeneous signal on MRI, lipomas are homogeneous |
| Epidermoid cyst | Epidermoids restrict on diffusion-weighted imaging, lipomas do not |
| Arachnoid cyst | Arachnoid cysts follow CSF signal on all sequences, lipomas follow fat signal |
| Syringomyelia | Syrinx contains fluid, lipomas contain fat on imaging |
| Neurofibroma | Neurofibromas enhance with contrast, lipomas typically do not |
| Arteriovenous malformation | AVMs show flow voids on MRI, lipomas do not |