Spinal CSF leak¶
Summary
- Spinal CSF leak is characterised by spontaneous or traumatic leakage of cerebrospinal fluid from the spinal dura
- Presents with orthostatic headaches, neck pain, and neurological symptoms
- Diagnosis relies on clinical presentation, imaging findings, and CSF analysis
Pathophysiology¶
- CSF leaks occur due to:
- Dural defects or weakness
- Traumatic injury to the spine
- Iatrogenic causes (e.g., lumbar puncture, spinal surgery)
- Results in intracranial hypotension and potential downward displacement of brain structures
- Compensatory mechanisms include venous engorgement and subdural fluid collections
Demographics¶
- Incidence: 5 per 100,000 per year
- More common in females (2:1 ratio)
- Peak age: 30-50 years
- Risk factors:
- Connective tissue disorders (e.g., Marfan syndrome, Ehlers-Danlos syndrome)
- Bone spurs or osteophytes
- Previous spinal surgery or intervention
Diagnosis¶
- Clinical presentation:
- Orthostatic headaches (worsening when upright, improving when supine)
- Neck pain or stiffness
- Tinnitus, hearing changes
- Visual disturbances
- Nausea and vomiting
- CSF analysis:
- Opening pressure typically low (<60 mm H2O)
- Normal or slightly elevated protein levels
- Normal glucose and cell count
- Myelography:
- Gold standard for localising CSF leaks
- CT or MR myelography can be used
Imaging¶
- MRI brain:
- Diffuse pachymeningeal enhancement
- Sagging of brain structures
- Venous engorgement
- Subdural fluid collections
- MRI spine:
- Extradural fluid collections
- Meningeal diverticula
- Nerve root sleeve cysts
- CT myelography:
- Contrast extravasation at leak site
- High sensitivity for detecting small leaks
- Digital subtraction myelography:
- Useful for dynamic imaging of CSF flow
- Can detect slow or intermittent leaks
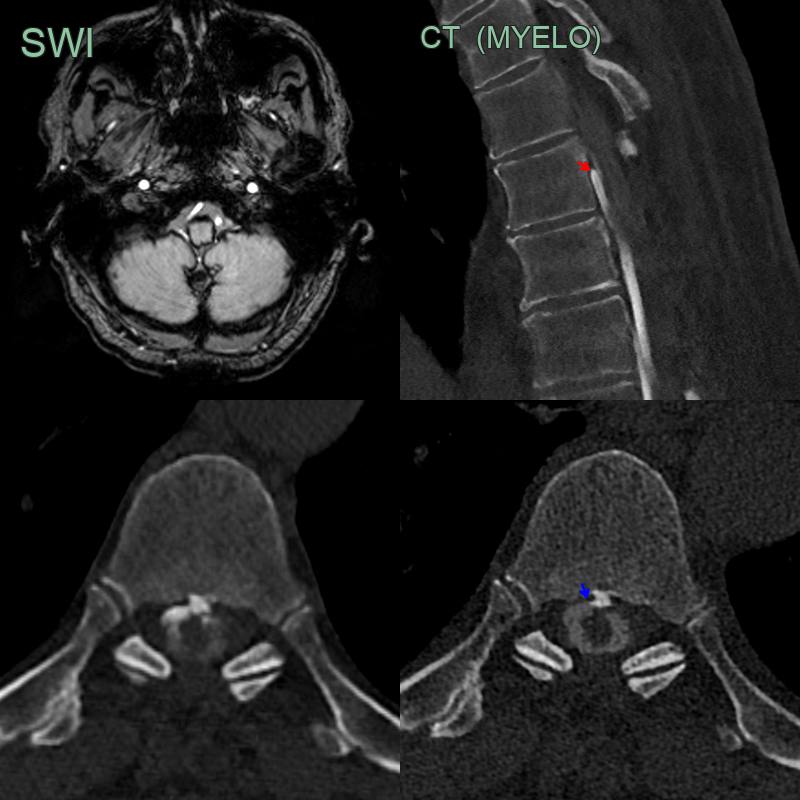
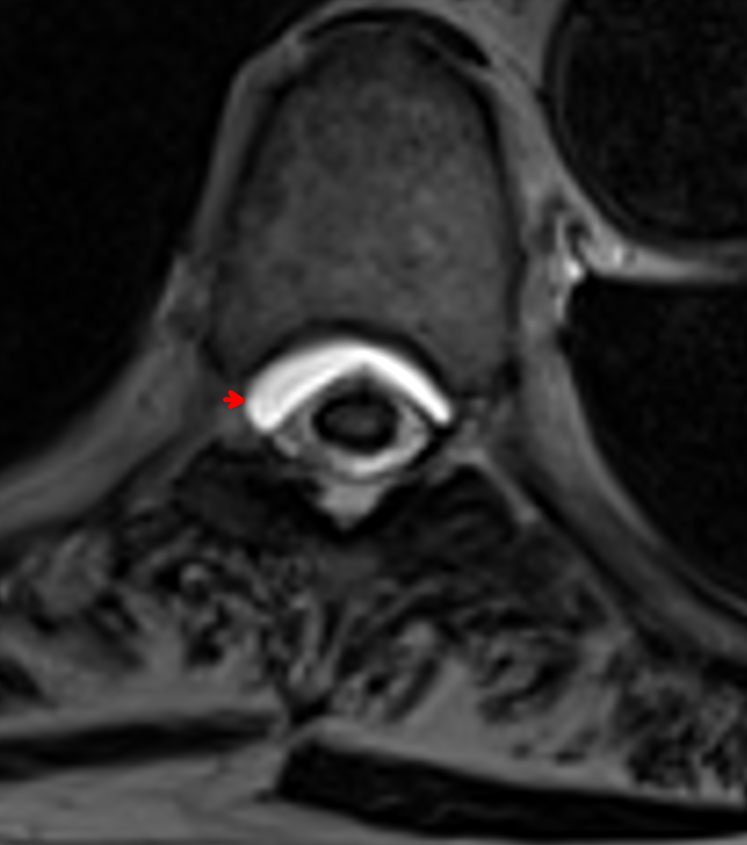
- 70-year-old patient with orthostatic headaches and transient bilateral 6th nerve palsies. The patient had a multi-level thoracic laminectomy for a compressive arachnoid cyst many years prior.
- CT myelography showed a rapidly filling small ventral epidural leak (red arrow).
- More apparent on later phase imaging, the ventral leak was associated with a small osteophyte (blue arrow).
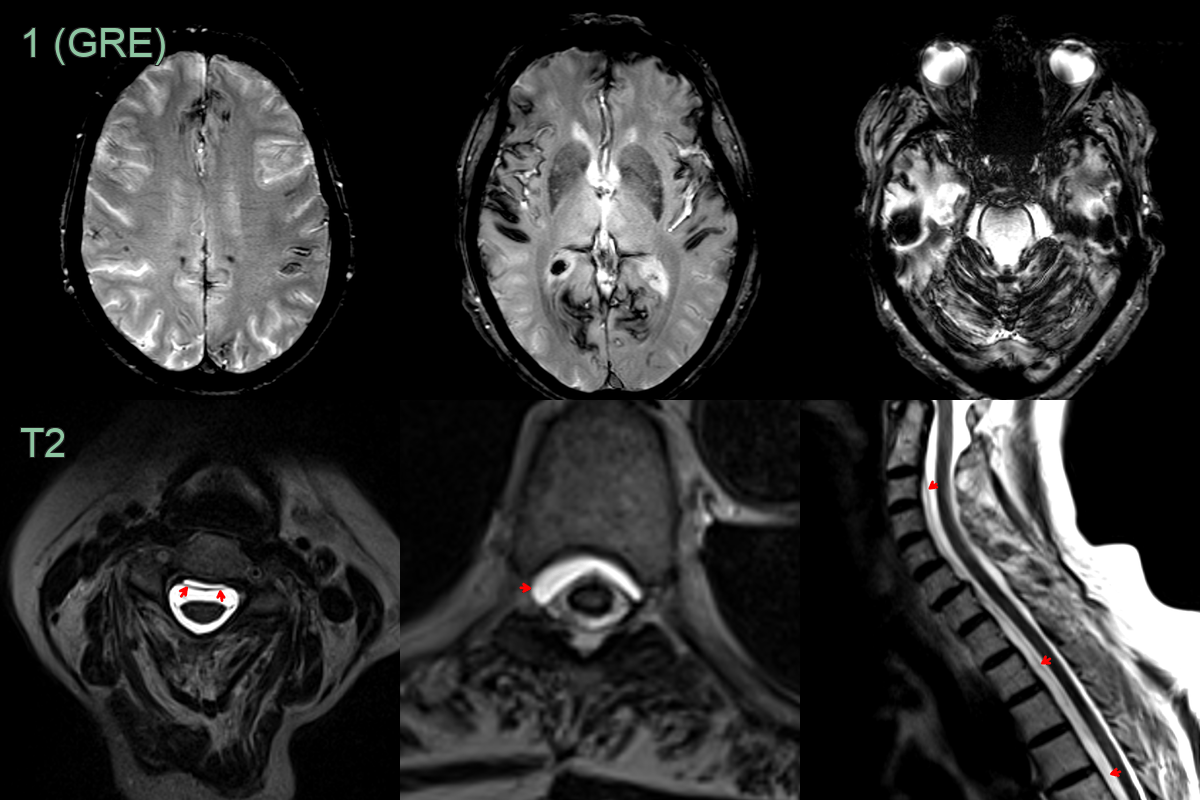
- A 70-year-old patient presented with tinnitus and dizziness.
- MRI showed extensive superficial siderosis above and below the tentorium.
- While the patient had no headache, given the distribution of siderosis, a CSF leak was suspected.
- MRI of the spine showed a longitudinally extensive ventral epidural collection, indicating a CSF leak.
Treatment¶
- Conservative management:
- Bed rest
- Hydration
- Caffeine intake
- Epidural blood patch:
- Autologous blood injection into epidural space
- Success rate: 30-70% after first attempt
- Targeted patching:
- Fibrin glue or blood patch at specific leak site
- Guided by imaging findings
- Surgical repair:
- Reserved for refractory cases
- Direct suturing of dural defect
- Duraplasty with autologous or synthetic grafts
- Follow-up imaging:
- MRI brain to assess resolution of intracranial hypotension signs
- Repeat myelography if symptoms persist
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Chiari malformation | Cerebellar tonsillar descent below the foramen magnum without diffuse pachymeningeal enhancement or brain sag |
| Subdural haematoma (primary) | Crescentic extra-axial collection with blood products but no pachymeningeal enhancement or brainstem sag |
| Diffuse dural disease (IgG4, neurosarcoidosis) | Nodular or asymmetric dural thickening; no brain sag or engorged venous structures |
| CSF-venous fistula | Myelogram shows filling of a paraspinal vein |