Spinal Haeangioblastoma¶
Summary
- Rare, benign vascular tumours of the central nervous system
- Most commonly occur in the cerebellum, but can affect the spinal cord
- Often associated with von Hippel-Lindau (VHL) disease
Pathophysiology¶
- Originate from mesenchymal cells of the capillary network
- Composed of stromal cells and abundant capillaries
- Tumour growth leads to cyst formation and oedema
- VHL gene mutation implicated in pathogenesis
Demographics¶
- Incidence: 1.5-2.1% of all spinal cord tumours
- Peak age: 20-40 years
- Male:Female ratio = 1.6:1
- 20-30% associated with VHL disease
Diagnosis¶
- Clinical presentation:
- Gradual onset of neurological symptoms
- Pain (radicular or local)
- Sensory disturbances
- Motor weakness
- Gait abnormalities
- Physical examination:
- Hyperreflexia
- Sensory level deficits
- Motor weakness
- Laboratory tests:
- Genetic testing for VHL mutations
- Elevated erythropoietin levels in some cases
Imaging¶
- MRI:
- T1-weighted: isointense to hypointense solid nodule
- T2-weighted: hyperintense cystic component, isointense nodule
- Contrast-enhanced T1: intense enhancement of solid nodule
- Flow voids may be visible
- Spinal angiography:
- Hypervascular tumour blush
- Enlarged feeding arteries
- Early venous drainage
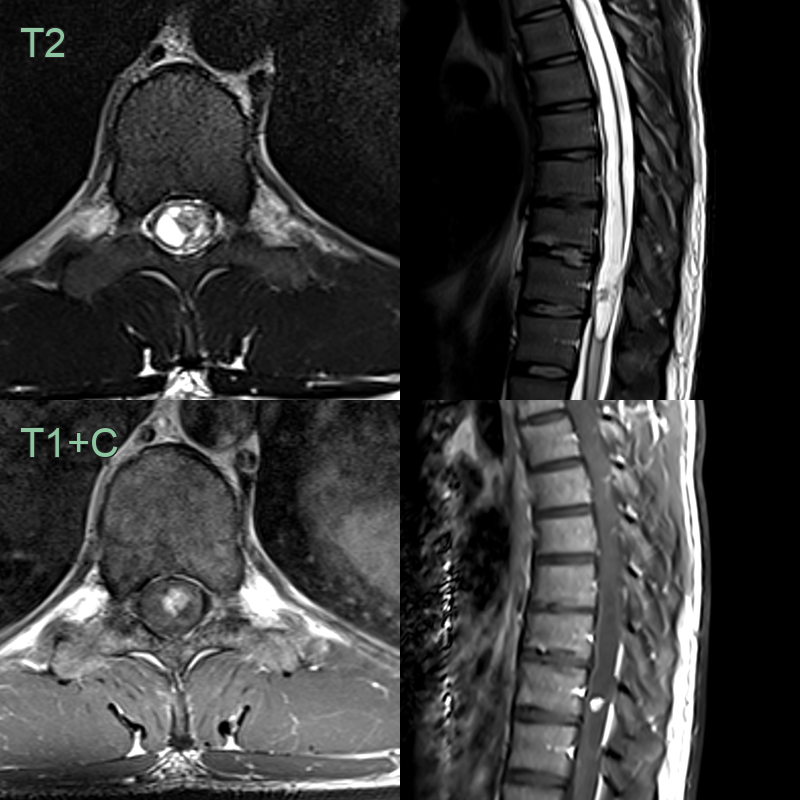
- 20-year-old patient presented with lower limb weakness and paraesthesia.
- MRI showed an avidly enhancing nodule distal to a longitudinally extensive syrinx.
Treatment¶
- Surgical resection:
- Complete excision is the goal
- Microsurgical techniques with intraoperative neurophysiological monitoring
- Preoperative embolization:
- May reduce intraoperative bleeding
- Controversial due to potential complications
- Radiation therapy:
- Reserved for inoperable cases or residual tumour
- Stereotactic radiosurgery for small, well-defined lesions
- Follow-up:
- Regular MRI surveillance
- Screening for VHL-associated tumours in affected patients
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Spinal Astrocytoma | Tends to be more infiltrative and less well-defined than hemangioblastomas |
| Spinal Cord Ependymoma | Lacks cystic component typically seen in hemangioblastomas |
| Idiopathic syringomyelia | Central fluid-filled cavity without an enhancing mural nodule |
| Spinal Schwannoma | Typically enhances homogeneously, unlike the nodular enhancement of hemangioblastomas |
| Spinal Metastasis | Often multiple lesions, whereas hemangioblastomas are usually solitary |
| Spinal Arteriovenous Malformation | Flow voids on MRI, not typically seen in hemangioblastomas |
| Spinal Cavernoma | Lacks the associated cyst seen in hemangioblastomas |