Sturge-Weber Syndrome¶
Summary
- Rare neurocutaneous disorder characterised by facial port-wine stain, leptomeningeal angioma, and glaucoma
- Caused by somatic mosaic mutation in GNAQ gene1
- Imaging findings include cerebral calcifications, cortical atrophy, and leptomeningeal enhancement
Pathophysiology¶
- Somatic activating mutation in GNAQ gene (c.548G>A, p.R183Q)1
- Leads to abnormal development of blood vessels in face, brain, and eye
- Results in:
- Facial port-wine stain (capillary malformation)
- Leptomeningeal angiomatosis
- Choroidal vascular malformation
Demographics¶
- Incidence: 1 in 20,000 to 50,000 live births2
- No gender predilection
- Typically sporadic, not inherited
- Presents at birth or early infancy
Diagnosis¶
- Clinical triad:
- Facial port-wine stain (usually in V1 distribution of trigeminal nerve)
- Leptomeningeal angioma
- Glaucoma
- Other features:
- Seizures (often refractory)
- Developmental delay
- Hemiparesis
- Visual field defects
Imaging¶
- CT findings:
- Gyriform calcifications in cerebral cortex
- Cortical atrophy
- Enlarged choroid plexus
- MRI findings:
- T1-weighted:
- Cortical atrophy
- Enlarged choroid plexus
- T2-weighted:
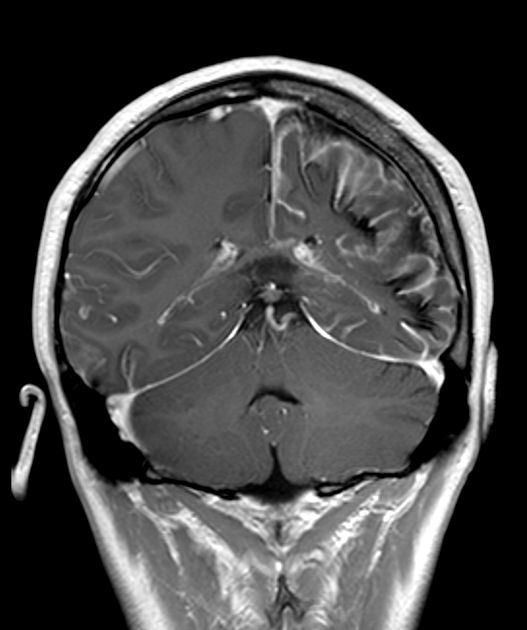
- Leptomeningeal enhancement
- White matter hypointensity (calcifications)
- Susceptibility-weighted imaging (SWI):
- Prominent cortical veins
- Gyriform calcifications
- Angiography:
- Leptomeningeal angiomatosis
- Abnormal cortical veins
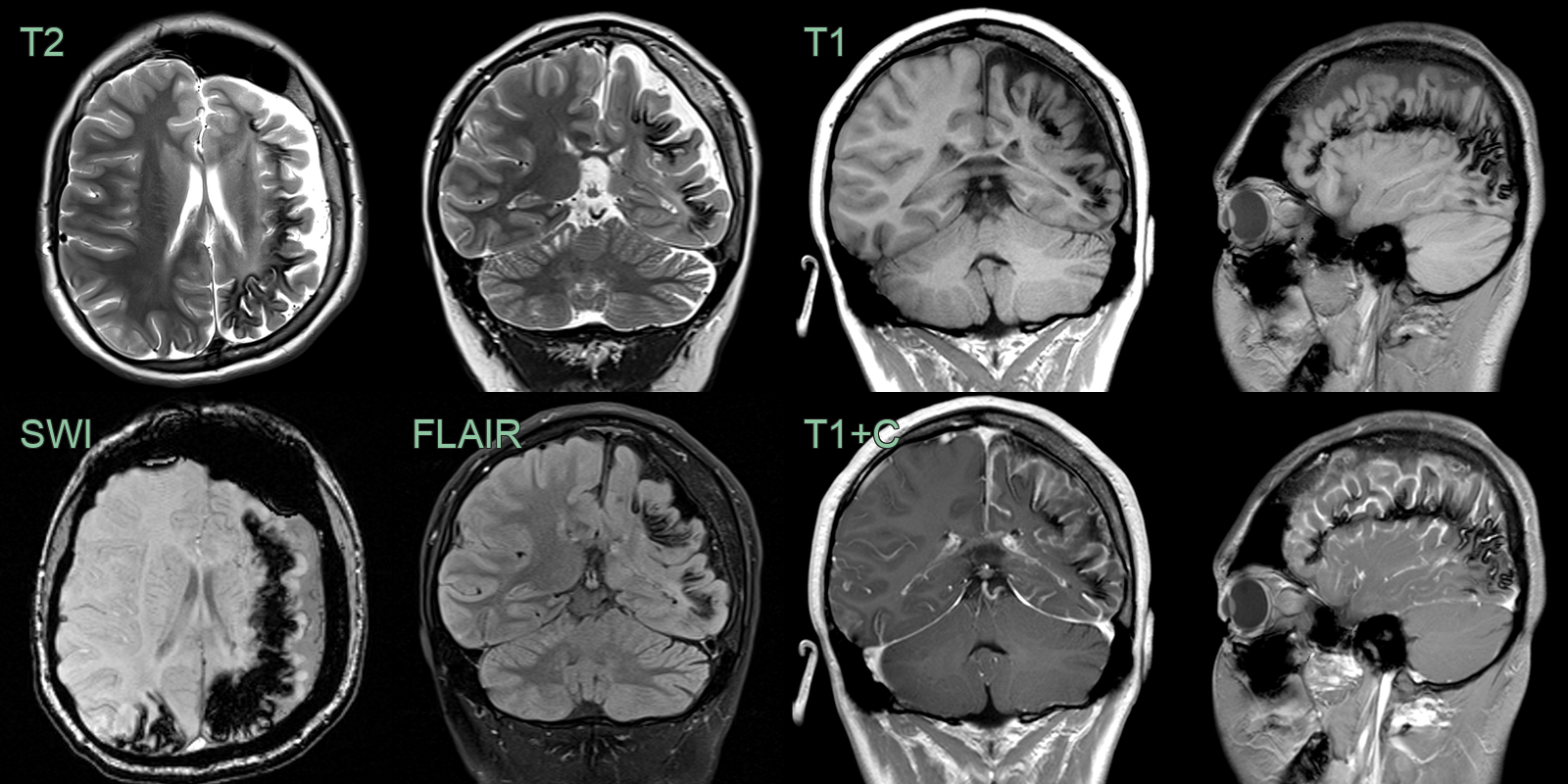
- 20-year-old patient with Struge-Weber syndrome has left sided hemiatrophy, cortical/subcortical calcification, enhancement in the leptomeningeal enhancement, calvarial hyperostosis and frontal sinus dilatation.
Treatment¶
- Multidisciplinary approach:
- Neurology: Anticonvulsants for seizure control
- Ophthalmology: Management of glaucoma
- Dermatology: Laser therapy for port-wine stain
- Surgical options:
- Hemispherectomy for refractory seizures3
- Focal resection of epileptogenic cortex
- Aspirin: May reduce stroke-like episodes4
- Endocrine management: For growth hormone deficiency and hypothyroidism
- Rehabilitation: Physical and occupational therapy for hemiparesis
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Dyke-Davidoff-Masson syndrome | Unilateral cerebral atrophy with calvarial thickening and ipsilateral sinus hyperpneumatisation; no gyriform calcifications or pial enhancement |
| Hemimegalencephaly | Unilateral hemispheric enlargement with cortical dysplasia; no leptomeningeal angiomatosis or pial enhancement |
| Tuberous sclerosis | Cortical tubers and subependymal nodules on MRI; calcifications on CT; no unilateral pial angioma or progressive cerebral atrophy |
| PHACE syndrome | Posterior fossa malformations (cerebellar hypoplasia, Dandy-Walker); ipsilateral large facial haemangioma; no leptomeningeal enhancement or gyriform calcifications |
| Cobb syndrome | Spinal rather than intracranial leptomeningeal vascular malformation; no ipsilateral cerebral atrophy or gyriform calcifications |
-
Shirley MD, et al. Sturge-Weber syndrome and port-wine stains caused by somatic mutation in GNAQ. N Engl J Med. 2013;368(21):1971-1979. PMID: 23656586 ↩↩
-
Comi AM. Presentation, diagnosis, pathophysiology, and treatment of the neurological features of Sturge-Weber syndrome. Neurologist. 2011;17(4):179-184. PMID: 21712663 ↩
-
Kossoff EH, et al. Hemispherectomy for intractable unihemispheric epilepsy: outcome in 26 patients. Neurology. 2003;61(11):1551-1558. PMID: 14663041 ↩
-
Lance EI, et al. Aspirin use in Sturge-Weber syndrome: side effects and clinical outcomes. J Child Neurol. 2013;28(2):213-218. PMID: 22850081 ↩