Subacute Combined Degeneration of the Cord (SACD)¶
Summary
- Neurological disorder caused by vitamin B12 deficiency
- Affects posterior and lateral columns of the spinal cord
- Characterised by symmetric demyelination and axonal loss
Pathophysiology¶
- Vitamin B12 deficiency leads to:
- Impaired methylation reactions in the central nervous system
- Accumulation of homocysteine and methylmalonic acid
- Demyelination and axonal degeneration in the spinal cord
- Primarily affects:
- Posterior columns (proprioception and vibration sense)
- Lateral corticospinal tracts (motor function)
- Spinocerebellar tracts (coordination)
Demographics¶
- Most common in:
- Elderly individuals
- Vegetarians and vegans
- Patients with malabsorption disorders (e.g., pernicious anaemia, Crohn's disease)
- Individuals with a history of gastric surgery
- No significant gender predilection
- Incidence increases with age
Diagnosis¶
- Clinical presentation:
- Symmetric paraesthesias and numbness in extremities
- Ataxia and impaired proprioception
- Progressive spastic paraparesis
- Cognitive impairment in advanced cases
- Laboratory findings:
- Low serum vitamin B12 levels (<200 pg/mL)
- Elevated homocysteine and methylmalonic acid levels
- Macrocytic anaemia (not always present)
- Neurophysiological studies:
- Abnormal somatosensory evoked potentials
- Reduced nerve conduction velocities
Imaging¶
- MRI findings:
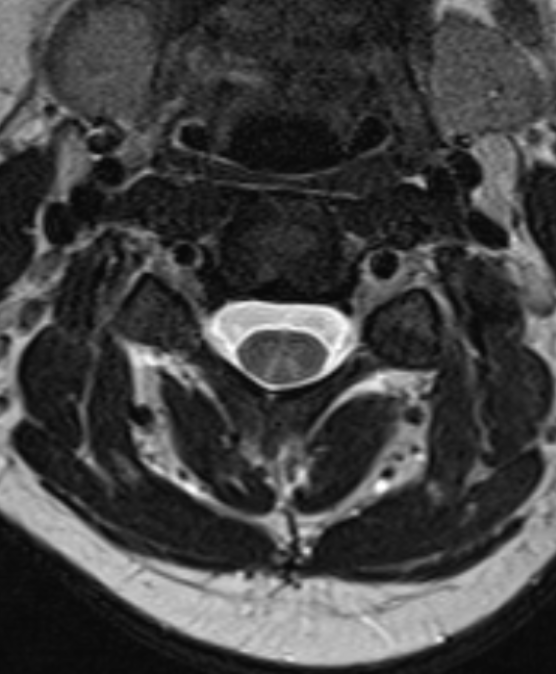
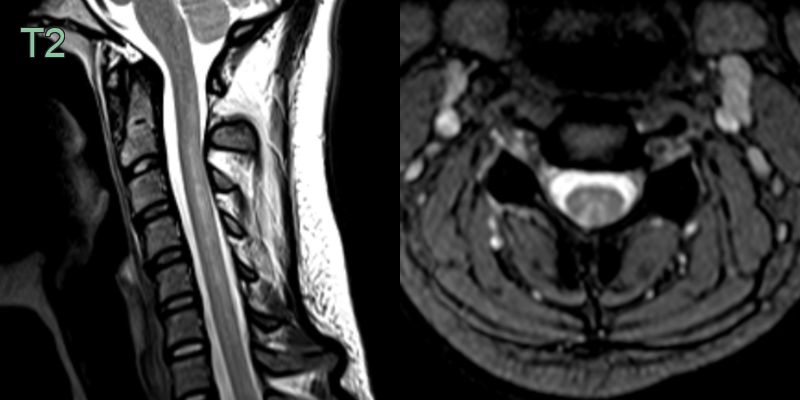
- T2-weighted and FLAIR hyperintensities in the posterior and lateral columns
- "Inverted V" or "rabbit ears" sign on axial images
- Cervical and thoracic cord involvement most common
- Contrast enhancement uncommon
- Spinal cord atrophy in chronic cases
- Diffusion-weighted imaging:
- May show restricted diffusion in acute stages
- Follow-up imaging:
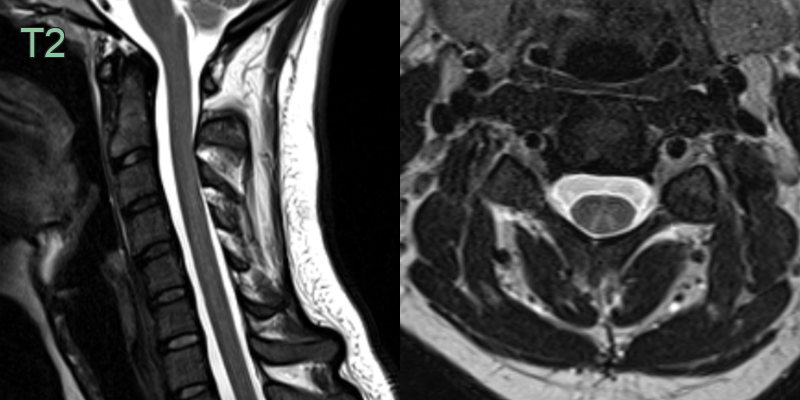
- Resolution of signal abnormalities with treatment
- 35-year-old patient presented with sensory ataxia.
- MRI showed an "inverted-V" corresponding to the dorsal columns in the cervical region.
- After B12 replacement, the patient's symptoms entirely resolved and the dorsal cord signal abnormality improved.
Treatment¶
- Vitamin B12 replacement therapy:
- Intramuscular injections: 1000 μg daily for 1 week, then weekly for 4-8 weeks, followed by monthly maintenance
- Oral supplementation: 1000-2000 μg daily (if absorption is not impaired)
- Treat underlying cause of B12 deficiency (e.g., pernicious anaemia)
- Supportive care:
- Physical therapy and rehabilitation
- Management of neurological complications
- Prognosis:
- Early diagnosis and treatment crucial for preventing irreversible neurological damage
- Improvement typically seen within 3-6 months of treatment initiation
- Some patients may have residual neurological deficits
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Multiple Sclerosis | Short cord lesions (<2 vertebral segments) with dorsolateral predilection; periventricular and juxtacortical brain plaques (Dawson's fingers); no inverted-V sign |
| Copper deficiency myelopathy | Identical dorsal column T2 signal and inverted-V pattern; indistinguishable from B12 deficiency on imaging alone |
| HTLV-1 associated myelopathy | Dorsal and lateral column T2 hyperintensity; thoracic cord atrophy; no inverted-V pattern |
| HIV vacuolar myelopathy | Posterior and lateral column involvement; associated cerebral white matter changes; thoracic cord predilection |
| Tabes dorsalis | Dorsal column T2 signal change; may appear identical to SCD on imaging; associated leptomeningeal enhancement |
| Neuromyelitis optica (NMO) | Longitudinally extensive T2 hyperintensity (≥3 vertebral segments); central cord; optic nerve lesions |
| Cervical Spondylotic Myelopathy | Structural cord compression from disc or osteophyte at compression level; lateral column and posterior column signal; no inverted-V pattern |
| Friedreich's Ataxia | Spinal cord atrophy with dorsal column T2 signal; cerebellar atrophy; no inverted-V pattern |