Subarachnoid Haemorrhage (SAH)¶
Summary
- Acute bleeding into the subarachnoid space
- Typically presents with sudden, severe headache ("thunderclap headache")
- CT is the initial imaging modality of choice, with CSF analysis if CT is negative
Pathophysiology¶
- Rupture of intracranial aneurysm (80-85% of cases)
- Non-aneurysmal causes:
- Arteriovenous malformations
- Perimesencephalic haemorrhage
- Vasculitis
- Cerebral venous thrombosis
- Complications:
- Rebleeding
- Vasospasm
- Hydrocephalus
- Seizures
Demographics¶
- Incidence: 6-10 per 100,000 person-years
- Mean age of onset: 50-60 years
- Female predominance (1.6:1)
- Risk factors:
- Hypertension
- Smoking
- Excessive alcohol consumption
- Family history of aneurysms
Diagnosis¶
- Clinical presentation:
- Sudden, severe headache
- Nausea and vomiting
- Neck stiffness
- Photophobia
- Altered consciousness
- Investigations:
- Non-contrast CT brain (sensitivity 98% within 12 hours)
- Lumbar puncture if CT negative (xanthochromia)
- CT angiography or digital subtraction angiography to identify source
Imaging¶
- Non-contrast CT brain:
- Hyperdense blood in subarachnoid spaces
- Intraventricular or intraparenchymal extension may be present
- Fisher grading scale for SAH severity
- CT angiography:
- Identification of aneurysms or vascular malformations
- Sensitivity 98% for aneurysms >3mm
- MRI:
- FLAIR sequence sensitive for subacute SAH
- SWI useful for detecting microbleeds
- Digital subtraction angiography:
- Gold standard for aneurysm detection
- Allows for treatment planning
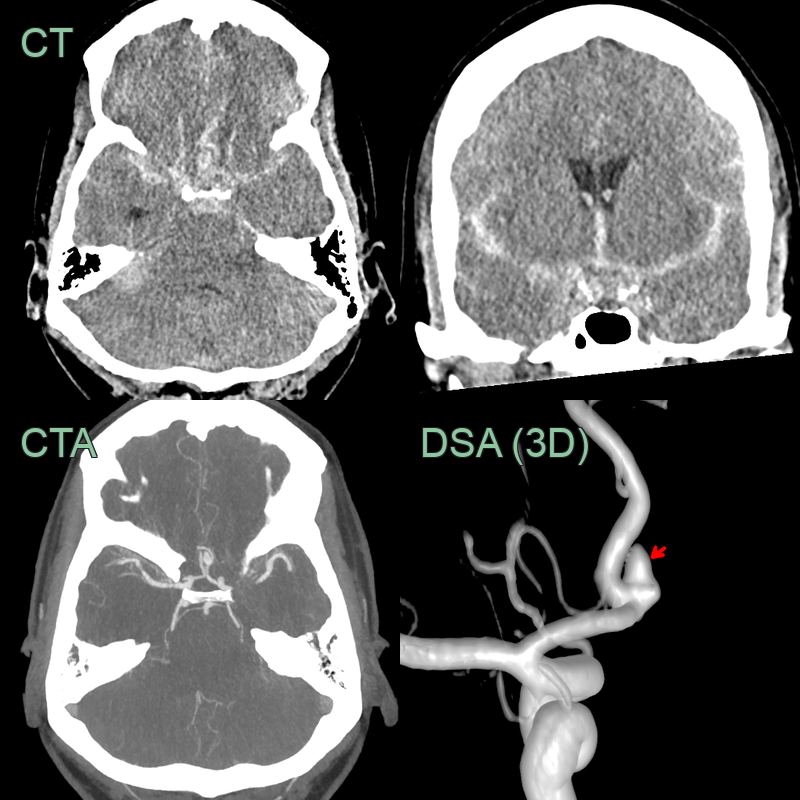
- 60-year-old patient presented obtunded.
- CT showed a large left supraclinoid ICA aneurysm with extensive basal cistern subarachnoid haemorrhage and acute hydrocephalus.
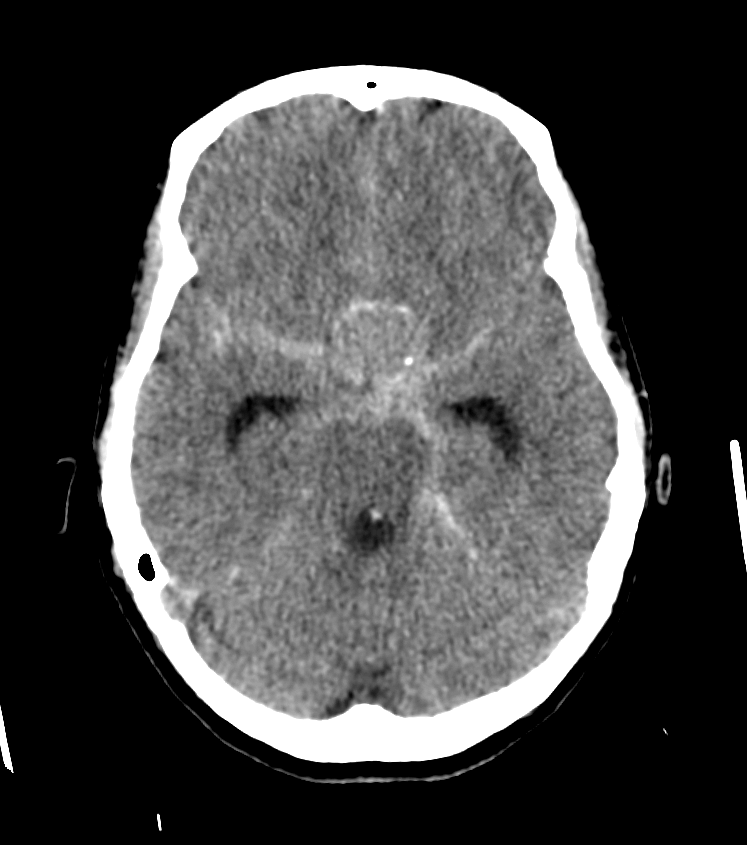
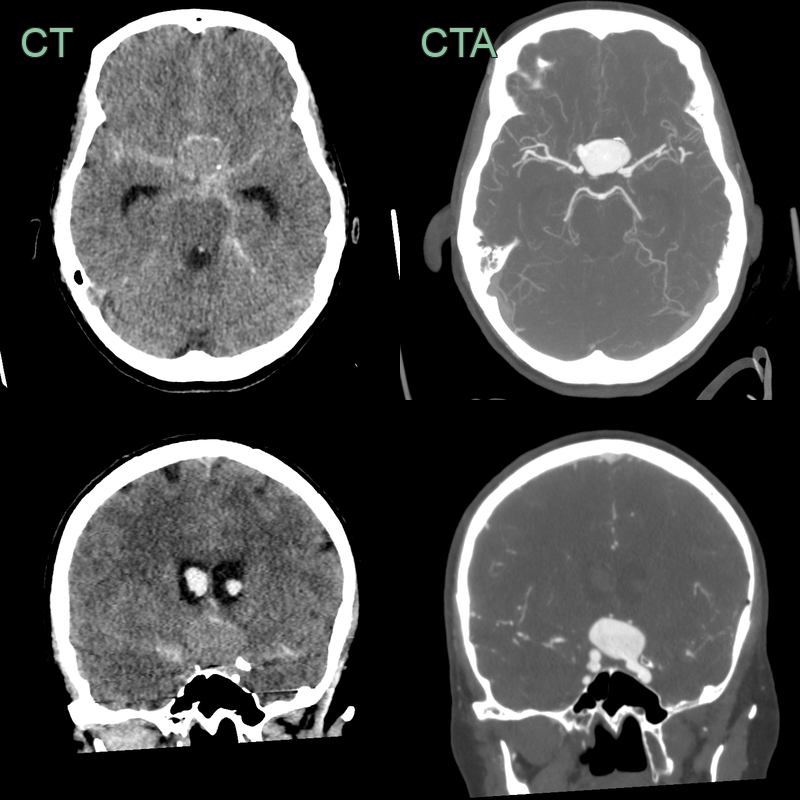
- A 60-year-old patient presented with headache and reduced GCS.
- CT showed diffuse symmetrical subarachnoid haemorrhage centred on the suprasellar space.
- CTA and 3D rotation DSA showed a 4 mm anterior communicating aneurysm.
Treatment¶
- Initial management:
- Airway protection and haemodynamic stabilisation
- Blood pressure control (target SBP <160 mmHg)
- Nimodipine for vasospasm prevention
- Aneurysm treatment:
- Endovascular coiling: preferred for most aneurysms
- Surgical clipping: may be preferred for some complex aneurysms
- Management of complications:
- External ventricular drainage for hydrocephalus
- Induced hypertension for delayed cerebral ischaemia
- Anticonvulsants for seizure prophylaxis (controversial)
- Rehabilitation and long-term follow-up:
- Neuropsychological assessment
- Screening for depression and anxiety
- Follow-up imaging to assess for aneurysm recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Pseudo-subarachnoid haemorrhage | Diffuse sulcal hyperdensity on CT due to severe cerebral oedema or hypoxic-ischaemic injury; no aneurysm on CTA; resolves with treatment of underlying cause |
| Convexity SAH from RCVS | Peripheral cortical sulcal blood rather than basilar cistern predominance; multifocal arterial beading on MRA; typically bilateral and small |
| Convexity SAH from cerebral venous thrombosis | Venous sinus or cortical vein filling defect on CT/MR venography; associated venous infarction crossing arterial territories |
| Pituitary apoplexy | Haemorrhage confined to pituitary fossa on MRI; T1 hyperintensity within enlarged pituitary; no basal cistern blood |
| Intracerebral haemorrhage | Blood in brain parenchyma rather than subarachnoid space on CT; intraparenchymal T1 and T2 signal changes |
| Leptomeningeal carcinomatosis | Sulcal FLAIR hyperintensity without CT-hyperdense blood; nodular leptomeningeal enhancement on contrast MRI |