Subdural empyema
Summary
- Subdural empyema is a life-threatening intracranial infection characterised by purulent material accumulation between the dura mater and arachnoid membrane
- Most commonly results from complications of sinusitis, otitis media, or neurosurgical procedures
- Rapid diagnosis and treatment are crucial due to high morbidity and mortality rates
Pathophysiology
- Infection typically spreads from contiguous structures (e.g., sinuses, middle ear) or hematogenously
- Bacteria invade the subdural space, leading to:
- Inflammatory response
- Increased intracranial pressure
- Potential brain parenchyma compression
- Venous thrombosis and infarction
- Common pathogens:
- Streptococcus species
- Staphylococcus aureus
- Anaerobic bacteria
Demographics
- More common in males (2:1 male to female ratio)
- Peak incidence in second and third decades of life
- Higher prevalence in developing countries
- Risk factors:
- Recent sinusitis or otitis media
- Neurosurgical procedures
- Head trauma
- Immunocompromised state
Diagnosis
- Clinical presentation:
- Fever
- Headache
- Altered mental status
- Focal neurological deficits
- Seizures
- Laboratory findings:
- Elevated white blood cell count
- Increased C-reactive protein and erythrocyte sedimentation rate
- Lumbar puncture (if not contraindicated):
- Elevated protein
- Pleocytosis
- Normal or low glucose levels
- Blood cultures may be positive in some cases
Imaging
- Computed Tomography (CT):
- Hypodense, crescentic collection along the cerebral convexity
- Mass effect with midline shift
- Enhancement of the dura and leptomeninges
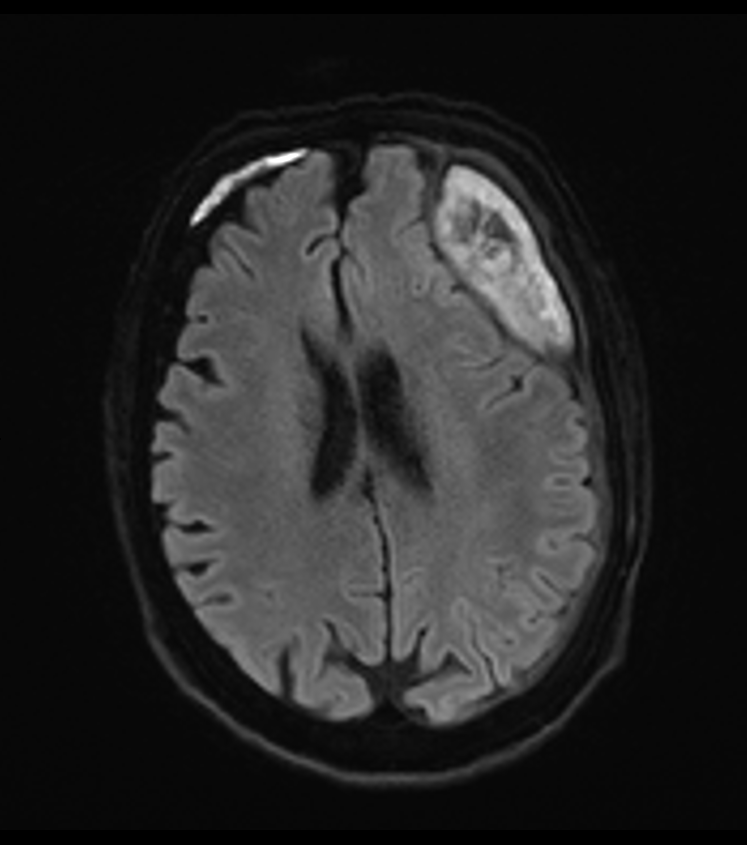
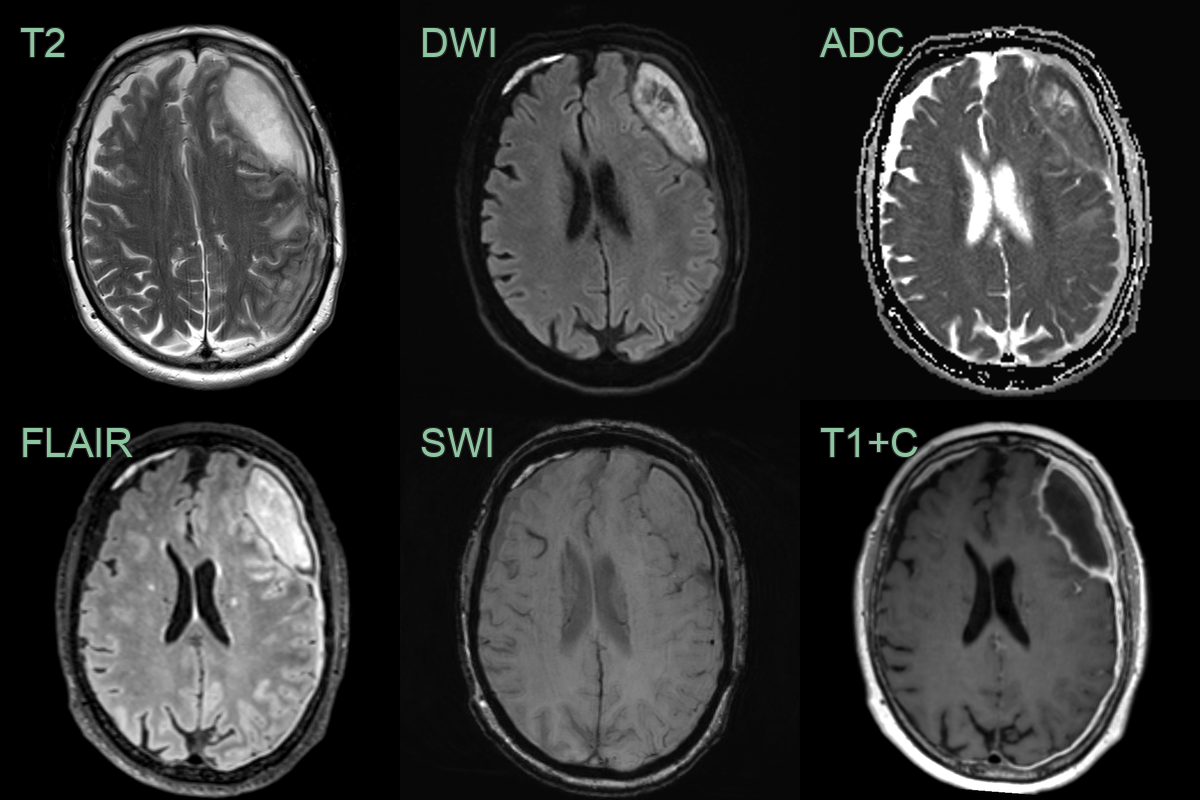
- Magnetic Resonance Imaging (MRI):
- Superior to CT for diagnosis and extent evaluation
- T1-weighted: iso- to hypointense collection
- T2-weighted: hyperintense collection
- Diffusion-weighted imaging: restricted diffusion
- Contrast-enhanced T1: rim enhancement
- Follow-up imaging is essential to monitor treatment response
Treatment
- Multidisciplinary approach involving neurosurgery, infectious disease, and radiology
- Empiric broad-spectrum intravenous antibiotics:
- Third-generation cephalosporin plus metronidazole
- Vancomycin if MRSA is suspected
- Surgical intervention:
- Craniotomy with evacuation of empyema
- Burr hole drainage in select cases
- Duration of antibiotic therapy:
- 4-6 weeks intravenous, followed by 2-4 weeks oral
- Management of underlying source (e.g., sinus surgery)
- Anticonvulsants for seizure prophylaxis
- Close monitoring for complications (e.g., cerebral venous thrombosis, brain abscess)
Differential diagnosis
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Brain abscess | Typically round or oval lesion on imaging, while subdural empyema is crescent-shaped |
| Epidural abscess | Located between dura and skull, not beneath dura; often associated with osteomyelitis |
| Subdural haematoma | No restricted diffusion; blood products showing T1 hyperintensity (subacute) or mixed signal; no rim enhancement |
| Meningitis | No localised extra-axial fluid collection on imaging; leptomeningeal rather than rim enhancement |
| Cerebral venous thrombosis | No pus collection; different imaging appearance with venous filling defects |
| Empyema-associated hydrocephalus | Ventricular enlargement present; empyema may be a secondary finding |
| Subgaleal abscess | Located outside the skull; no intracranial involvement on imaging |
| Cerebritis | Ill-defined area of cerebral oedema without discrete fluid collection |
| Encephalitis | Diffuse brain involvement; no localised fluid collection |
| Subdural effusion | No enhancement on contrast imaging; usually sterile fluid collection |