Subdural Haematoma¶
Summary
- Subdural haematoma (SDH) is a collection of blood between the dura and arachnoid layers of the meninges
- Typically results from tearing of bridging veins due to trauma or spontaneously in anticoagulated patients
- Imaging findings vary based on age of haematoma, with characteristic crescent-shaped extra-axial collection on CT/MRI
Pathophysiology¶
- Bridging veins traverse from cortical surface to dural venous sinuses
- Rupture of these veins leads to bleeding into subdural space
- Acute SDH: Fresh blood collection
- Subacute SDH: Liquefaction and breakdown of blood products (3-21 days)
- Chronic SDH: Encapsulated collection with osmotically driven fluid accumulation (>21 days)
Demographics¶
- Bimodal age distribution:
- Young adults: Often due to trauma
- Elderly: Increased risk due to brain atrophy and anticoagulation use
- Male predominance (3:1 male to female ratio)
- Risk factors:
- Trauma
- Anticoagulation therapy
- Alcohol abuse
- Coagulopathies
Diagnosis¶
- Clinical presentation:
- Acute: Headache, altered mental status, focal neurological deficits
- Chronic: Gradual onset of symptoms, cognitive decline, gait disturbances
- Physical examination:
- Pupillary abnormalities
- Hemiparesis
- Increased intracranial pressure signs
- Laboratory tests:
- Coagulation profile
- Complete blood count
Imaging¶
- CT (non-contrast):
- Acute: Hyperdense crescent-shaped collection
- Subacute: Isodense to brain parenchyma
- Chronic: Hypodense collection
- Mass effect and midline shift may be present
- MRI:
- Superior to CT for isodense subacute SDH
- T1WI:
- Acute: Isointense to hypointense
- Subacute: Hyperintense
- Chronic: Hypointense
- T2WI:
- Variable signal intensity based on age
- FLAIR: Hyperintense in all stages
- DWI: May show restricted diffusion in acute stage
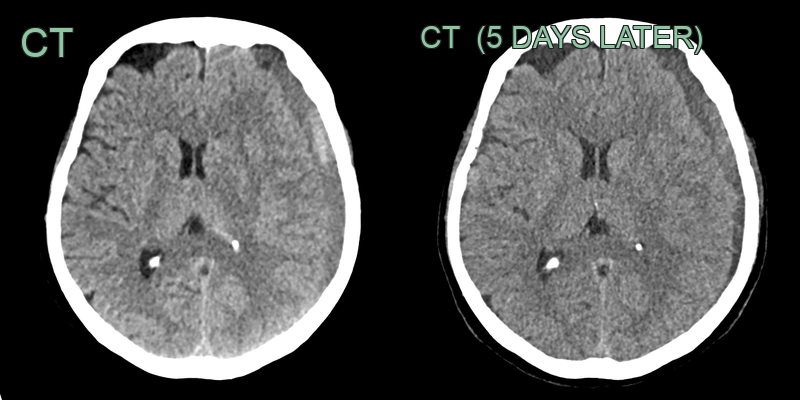
- 70-year-old patient presented with slurred speech and confusion (although no history of trauma).
- CT showed a mixed hyper- and hypo-dense cresentic collection over the left cerebral convexity.
- Mass effect caused distortion of the left lateral ventricle and minimal midline shift.
- 5 days later, the density of the acute blood decreased.
Treatment¶
- Conservative management:
- Small, asymptomatic SDH
- Serial imaging and neurological monitoring
- Surgical intervention:
- Indications: Large volume, significant mass effect, neurological deterioration
- Options:
- Burr hole drainage: Preferred for chronic SDH
- Craniotomy: For acute SDH or recurrent chronic SDH
- Medical management:
- Reversal of anticoagulation if applicable
- Seizure prophylaxis
- Osmotic therapy for increased intracranial pressure
- Prognosis:
- Depends on size, location, age of patient, and time to treatment
- Mortality rates: 20-30% for acute SDH, 3-13% for chronic SDH
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Epidural Haematoma | Lenticular shape on CT, does not cross suture lines |
| Subarachnoid Haemorrhage | Blood in subarachnoid space, often in basal cisterns |
| Empyema | Rim-enhancing extra-axial collection with restricted diffusion on DWI; no blood products on MRI |
| Arachnoid Cyst | No mass effect, CSF density on CT |