Subdural Hygroma¶
Summary
- Subdural hygroma is a collection of cerebrospinal fluid (CSF) in the subdural space without blood
- Often occurs following head trauma or neurosurgical procedures
- Imaging shows a crescent-shaped, extra-axial fluid collection with CSF density on CT and CSF signal characteristics on MRI
Pathophysiology¶
- Proposed mechanisms include:
- Tearing of arachnoid membrane, allowing CSF to enter subdural space
- Redistribution of CSF due to altered CSF dynamics
- Expansion of subdural space due to brain atrophy or decreased intracranial pressure
- May resolve spontaneously or progress to chronic subdural haematoma
Demographics¶
- Can occur in all age groups
- More common in:
- Elderly patients with brain atrophy
- Infants with traumatic birth or child abuse
- Patients following neurosurgical procedures or head trauma
Diagnosis¶
- Often asymptomatic and discovered incidentally
- When symptomatic, may present with:
- Headache
- Altered mental status
- Focal neurological deficits
- Seizures (rare)
- Clinical history of recent head trauma or neurosurgical intervention is important
Imaging¶
- CT findings:
- Hypodense, extra-axial, crescent-shaped fluid collection
- Density similar to CSF (0-20 Hounsfield units)
- No enhancement with contrast
- May cause mild mass effect
- MRI findings:
- T1: hypointense (isointense to CSF)
- T2: hyperintense (isointense to CSF)
- FLAIR: suppressed signal (unlike subdural haematoma)
- DWI: no restricted diffusion
- No enhancement on post-contrast images
- Differentiation from chronic subdural haematoma can be challenging
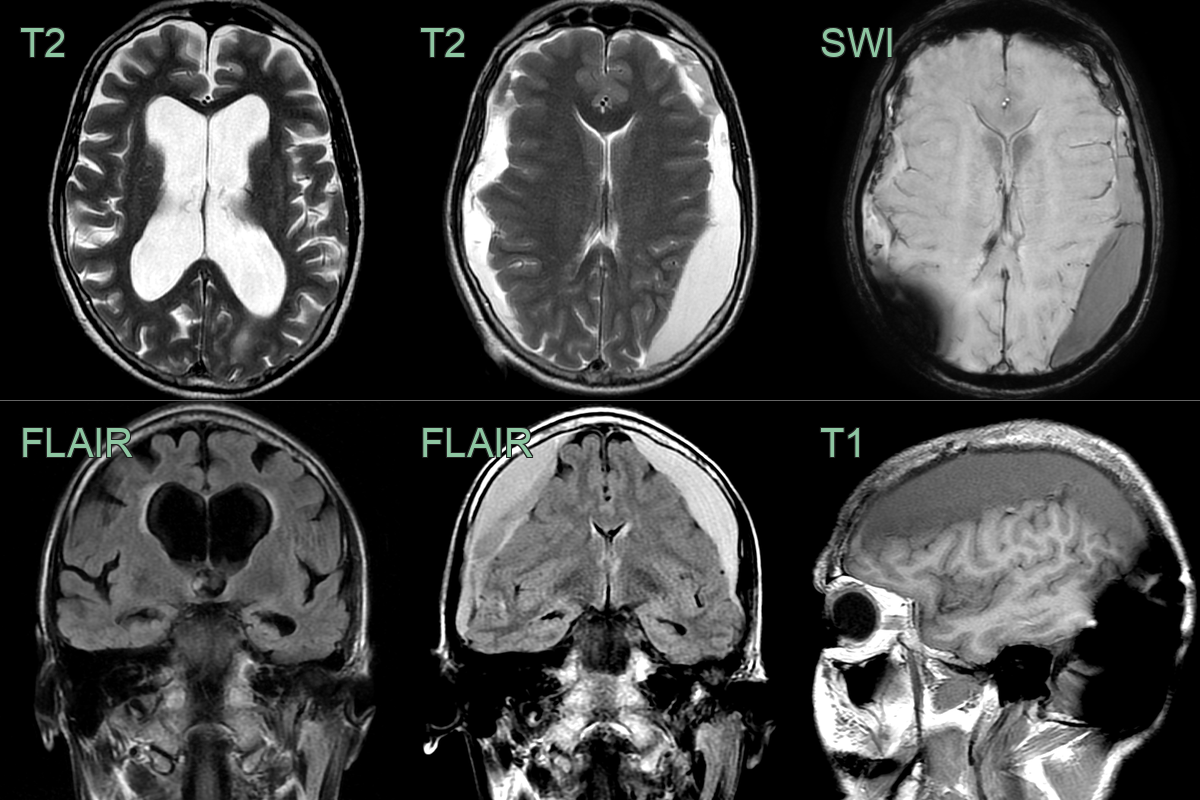
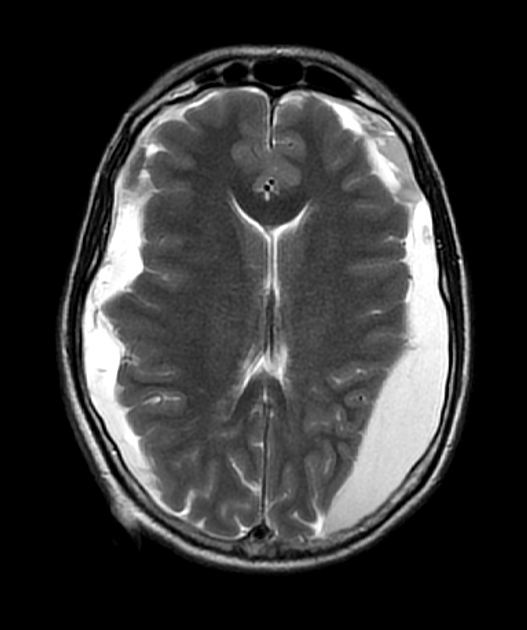
- A 70-year-old patient with gait disturbance and cognitive impairment underwent an intraventricular shunt for normal pressure hydrocephalus (albeit without classical imaging appearances).
- The patient had a persistent headache post-operatively. On the third post-operative day, an MRI showed bilateral subdural collections containing small regions of susceptibility (due to blood product) that resulted in effacement of the lateral ventricles.
Treatment¶
- Asymptomatic cases:
- Conservative management with close monitoring
- Serial imaging to assess for resolution or progression
- Symptomatic cases or significant mass effect:
- Surgical evacuation (burr hole drainage or craniotomy)
- Subdural-peritoneal shunt placement in recurrent cases
- Treat underlying cause (e.g., CSF leak repair)
- Address predisposing factors (e.g., anticoagulation management)
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Chronic Subdural Haematoma | Hygroma has lower density on CT; no blood products on MRI |
| Arachnoid Cyst | Hygroma follows CSF signal on all MRI sequences; arachnoid cyst may have different signal |
| Subdural Empyema | Empyema shows rim enhancement on contrast MRI and restricted diffusion; hygroma has no enhancement or DWI restriction |
| Epidural Haematoma | Hygroma is crescent-shaped and crosses sutures; epidural haematoma is typically biconvex and does not cross sutures |
| Cerebral Atrophy | Hygroma more likely to be focal; atrophy shows generalised sulcal widening with vessels in traversing the CSF space |