Superior Semicircular Canal Dehiscence Syndrome¶
Summary
- Rare inner ear disorder characterised by absence of bone overlying the superior semicircular canal
- Presents with vestibular and auditory symptoms triggered by sound or pressure changes
- Diagnosis confirmed by high-resolution CT imaging of temporal bones
Pathophysiology¶
- Absence of bone over superior semicircular canal creates a "third window" in the inner ear
- Abnormal communication between inner ear and middle cranial fossa
- Results in:
- Pressure-induced displacement of endolymph
- Abnormal activation of vestibular system
- Altered sound transmission to cochlea
Demographics¶
- Prevalence estimated at 0.5-2% in general population
- Typically presents in middle-aged adults (40-50 years)
- No significant gender predilection
- Bilateral involvement in 25-50% of cases
Diagnosis¶
- Clinical presentation:
- Vertigo and oscillopsia induced by loud sounds (Tullio phenomenon)
- Autophony (hearing one's own voice abnormally loud)
- Pulsatile tinnitus
- Chronic disequilibrium
- Diagnostic tests:
- Vestibular evoked myogenic potentials (VEMPs) with lowered thresholds
- Audiometry showing low-frequency air-bone gap
- Fistula test may be positive
Imaging¶
- High-resolution CT of temporal bones:
- Key diagnostic modality
- Axial and coronal planes with <1mm slice thickness
- Findings:
- Absence of bone over superior semicircular canal
- Direct communication between inner ear and middle cranial fossa
- MRI:
- May show fluid signal extending from superior semicircular canal to middle cranial fossa
- Useful for ruling out other causes of vestibular symptoms
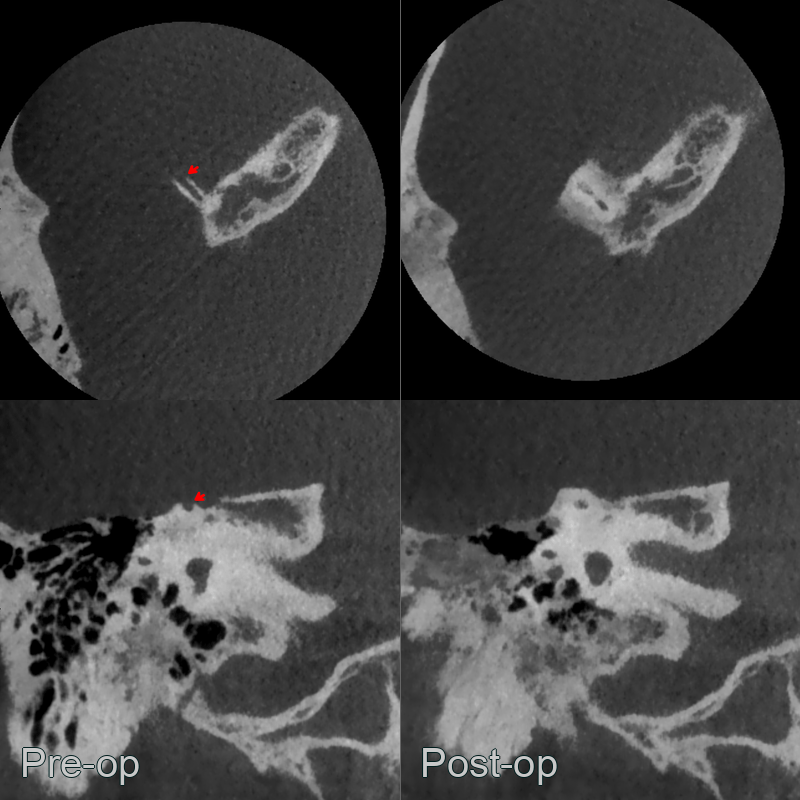
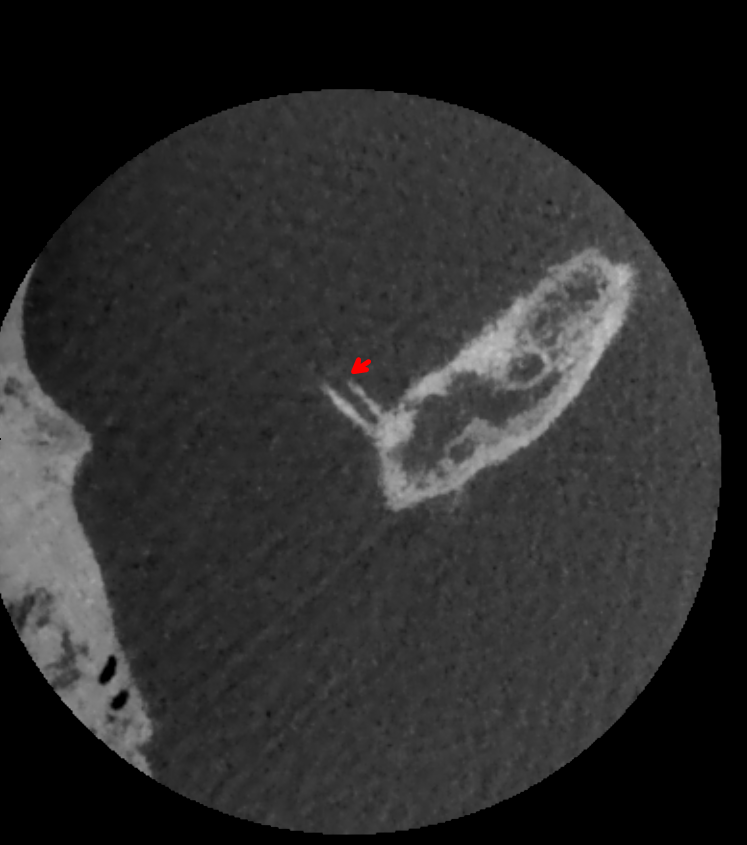
- A 30-year-old patient presented with noise-induced dizziness.
- Cone beam CT showed dehisence of the right superior semicircular canal.
- The dehisence resolved following a transmastoid resurfacing with bone pate.
Treatment¶
- Conservative management:
- Avoidance of symptom-triggering activities
- Vestibular rehabilitation
- Surgical options:
- Canal plugging: Occlusion of dehiscent canal with bone wax or fascia
- Resurfacing: Repair of dehiscence with cartilage, fascia, or bone graft
- Middle fossa craniotomy approach most common
- Outcomes:
- Surgical success rates of 80-90% for symptom improvement
- Potential complications include sensorineural hearing loss and vestibular dysfunction
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Tegmen tympani dehiscence | Bony defect in the tegmen tympani (roof of middle ear) rather than the superior semicircular canal arch on CT; different anatomical location |
| Superior canal thinning (without dehiscence) | Thin but intact bone covering the superior canal on thin-section CT; no true gap; partial volume averaging artefact |
| Enlarged vestibular aqueduct syndrome | Enlarged endolymphatic duct >1.5 mm at midpoint measurement on CT; cochlear involvement |
| Otosclerosis | Lucent halo around cochlea ("halo sign") on CT; fenestral or retrofenestral involvement; no dehiscence of semicircular canal |
| Cholesteatoma | Expansile soft tissue mass with bone erosion in middle ear or mastoid on CT; opacification of middle ear |