Susac Syndrome¶
Summary
- Rare autoimmune microangiopathy affecting the brain, retina, and inner ear
- Characterised by encephalopathy, branch retinal artery occlusions, and hearing loss
- Diagnosis relies on clinical triad and characteristic MRI findings
Pathophysiology¶
- Autoimmune-mediated endotheliopathy affecting small arteries
- Microinfarcts in the corpus callosum, retina, and cochlea
- Exact aetiology unknown, but likely involves anti-endothelial cell antibodies
Demographics¶
- Predominantly affects young women (20-40 years old)
- Male to female ratio approximately 1:3
- Rare condition with an estimated incidence of 0.14 per 100,000 person-years
Diagnosis¶
- Clinical triad:
- Encephalopathy
- Branch retinal artery occlusions
- Sensorineural hearing loss
- Often presents with incomplete triad initially
- Diagnostic criteria:
- At least two of the three clinical manifestations
- Characteristic MRI findings
- Exclusion of other differential diagnoses
Imaging¶
- MRI brain:
- Characteristic 'snowball' lesions in the corpus callosum
- Multiple small (3-7 mm) T2/FLAIR hyperintense lesions
- Lesions involve central fibres of corpus callosum, sparing the periphery
- Leptomeningeal enhancement may be present
- Fluorescein angiography:
- Branch retinal artery occlusions
- Arterial wall hyperfluorescence
- Optical coherence tomography:
- Retinal thinning in areas of infarction
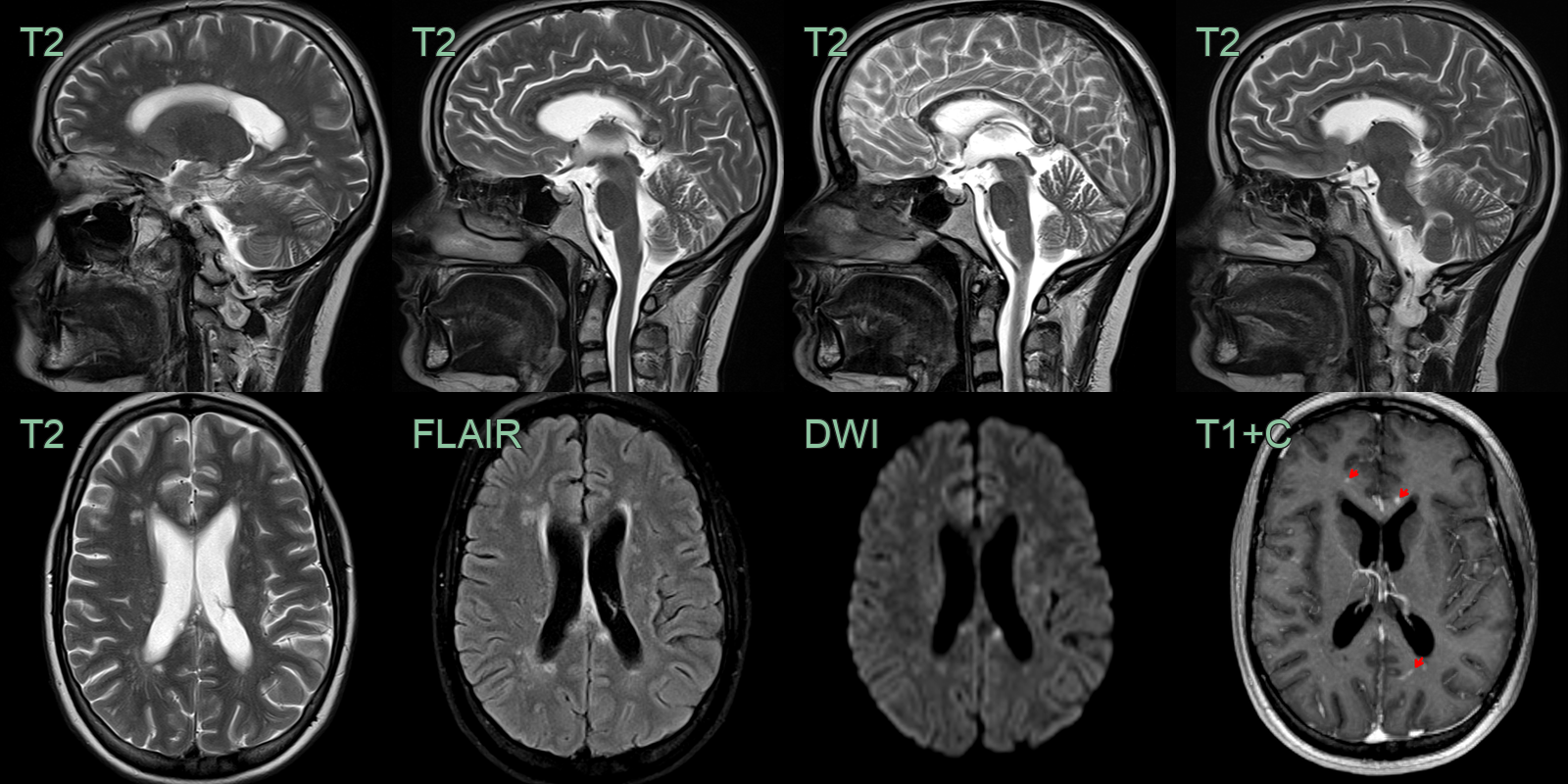
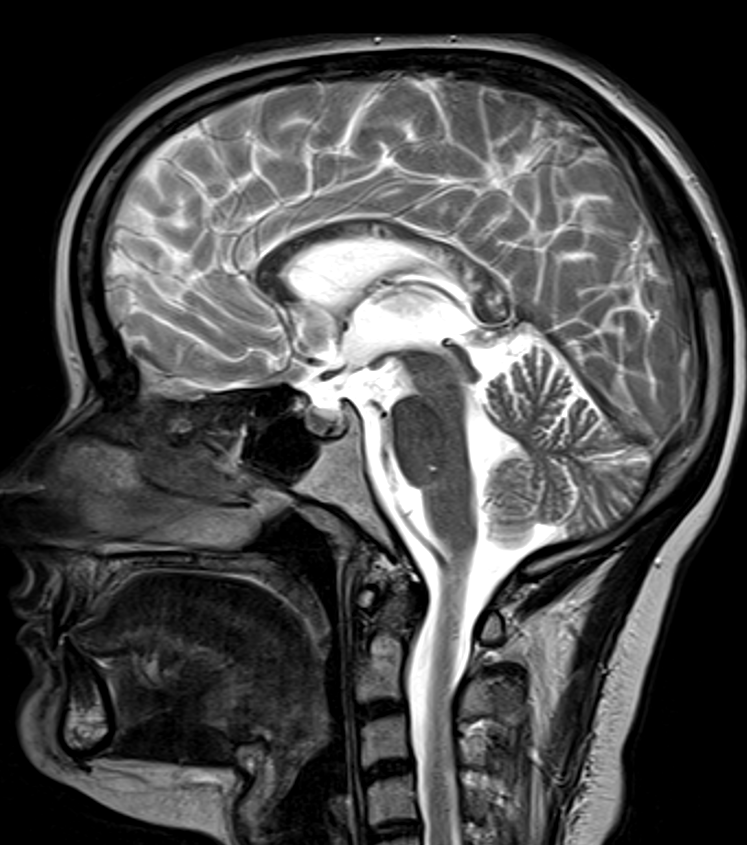
- A 30-year-old patient presented with a sensorineural hearing loss.
- MRI showed hyperintensities, some of which enhanced, within cerebral white matter with particular involvement of the corpus callosum.
Treatment¶
- Early diagnosis and aggressive immunosuppression crucial
- First-line therapy:
- High-dose intravenous methylprednisolone followed by oral prednisolone
- Intravenous immunoglobulin (IVIG)
- Second-line therapy:
- Cyclophosphamide
- Rituximab
- Mycophenolate mofetil
- Maintenance therapy:
- Low-dose prednisolone
- Mycophenolate mofetil or azathioprine
- Symptomatic management:
- Antiepileptic drugs for seizures
- Hearing aids for hearing loss
- Aspirin for antithrombotic effect
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Multiple sclerosis | Calloso-septal interface lesions (Dawson fingers) at the undersurface of the corpus callosum rather than central fibres; periventricular and juxtacortical ovoid plaques; no cortical microinfarcts |
| Acute disseminated encephalomyelitis | Large bilateral confluent T2 lesions involving grey and white matter; posterior fossa and basal ganglia involvement; no central corpus callosum "snowball" lesions |
| CNS vasculitis | Cortical and subcortical microinfarcts in multiple vascular territories; vessel wall enhancement on high-resolution MRI; no central corpus callosum predilection |
| Lyme neuroborreliosis | Periventricular and subcortical white matter T2/FLAIR lesions similar to MS; cranial nerve and meningeal enhancement; no central corpus callosum snowball pattern |