Sylvian aqueduct stenosis¶
Summary

- Sylvian aqueduct stenosis is a congenital or acquired narrowing of the cerebral aqueduct
- Results in obstructive hydrocephalus due to impaired CSF flow from the third to fourth ventricle
- Characterised by ventriculomegaly on imaging, with a dilated third ventricle and normal-sized fourth ventricle
Pathophysiology¶
- Congenital causes:
- Developmental abnormalities of the aqueduct
- Genetic factors (e.g., X-linked hydrocephalus)
- Acquired causes:
- Inflammation or infection (e.g., toxoplasmosis, viral infections)
- Tumours compressing the aqueduct
- Haemorrhage or gliosis
- Results in:
- Increased intracranial pressure
- Progressive ventriculomegaly
- Potential neurological deficits
Demographics¶
- Congenital form:
- More common in males (X-linked hydrocephalus)
- Often diagnosed prenatally or in early infancy
- Acquired form:
- Can occur at any age
- Incidence increases with age due to higher risk of tumours and vascular events
Diagnosis¶
- Clinical presentation:
- Infants: macrocephaly, bulging fontanelle, developmental delay
- Adults: headache, gait disturbances, cognitive decline, urinary incontinence
- Neurological examination:
- Papilledema
- Upward gaze palsy (Parinaud syndrome)
- Ataxia
- Ophthalmological assessment:
- Fundoscopy to evaluate for papilledema
Imaging¶
- CT:
- Ventriculomegaly of lateral and third ventricles
- Normal-sized fourth ventricle
- Possible periventricular hypodensity (transependymal CSF absorption)
- MRI:
- Gold standard for diagnosis
- T1-weighted and T2-weighted sequences:
- Dilated lateral and third ventricles
- Narrowed or obliterated aqueduct
- Normal-sized fourth ventricle
- CISS/FIESTA sequences:
- High-resolution imaging of the aqueduct
- Phase-contrast MRI:
- Evaluation of CSF flow dynamics
- Cine MRI:
- Demonstrates aqueductal CSF flow obstruction
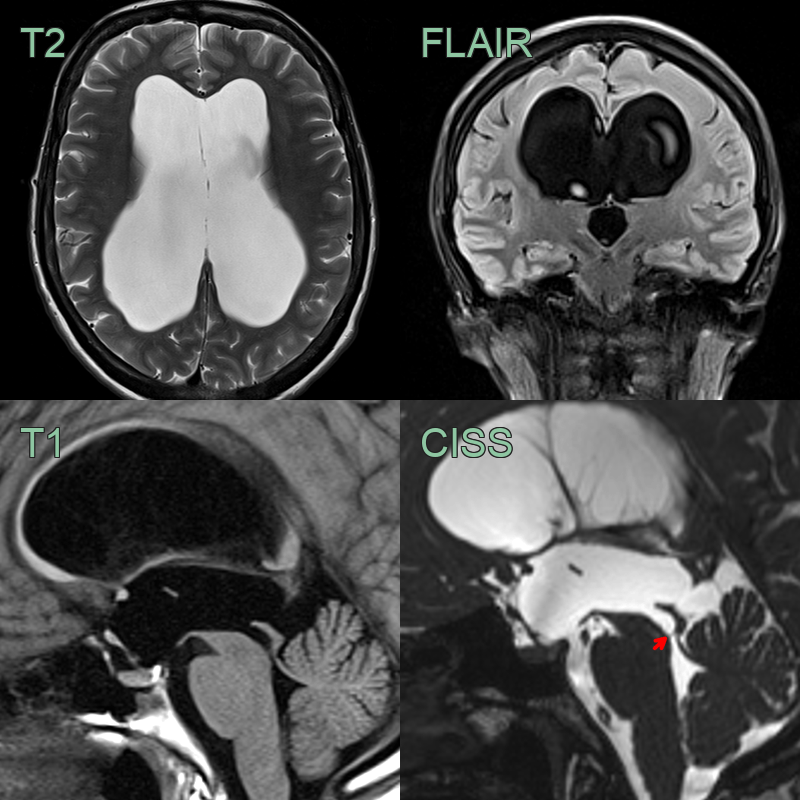
- A 50-year-old patient had progressive gait disturbance and more recent upper limb clumsiness.
- The lateral and third ventricles were very enlarged without periventricular oedema.
- A web in the inferior Sylvian aqueduct, better seen on CISS than T1 (red arrow), was causing impaired CSF outflow.
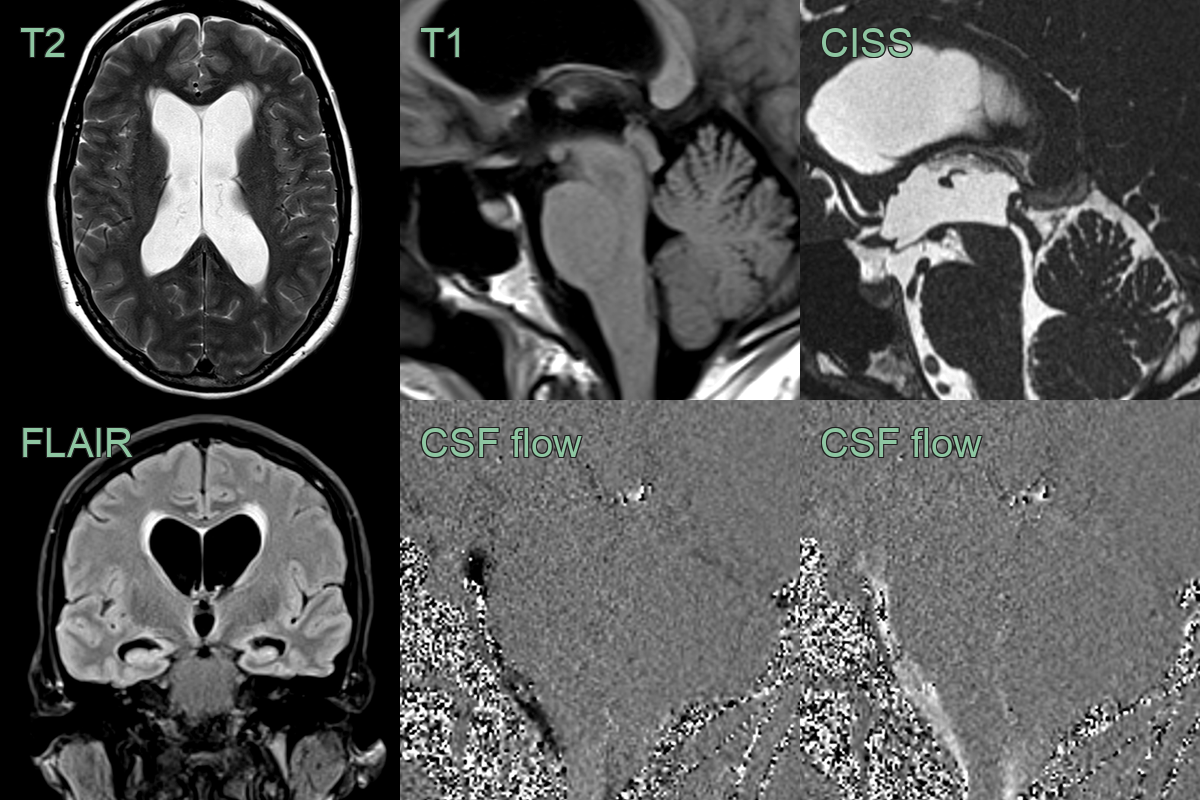
- A 50 year old presented with a chronic headache and gait disturbance.
- MRI showed ventriculomegaly with a periventricular rim of T2-hyperintense oedema.
- CISS imaging showed a filling defect in the superior Sylvian aqueduct likely to represent a web.
- CSF flow studies did not show pulsatile CSF flow across through the Sylvian aqueduct.
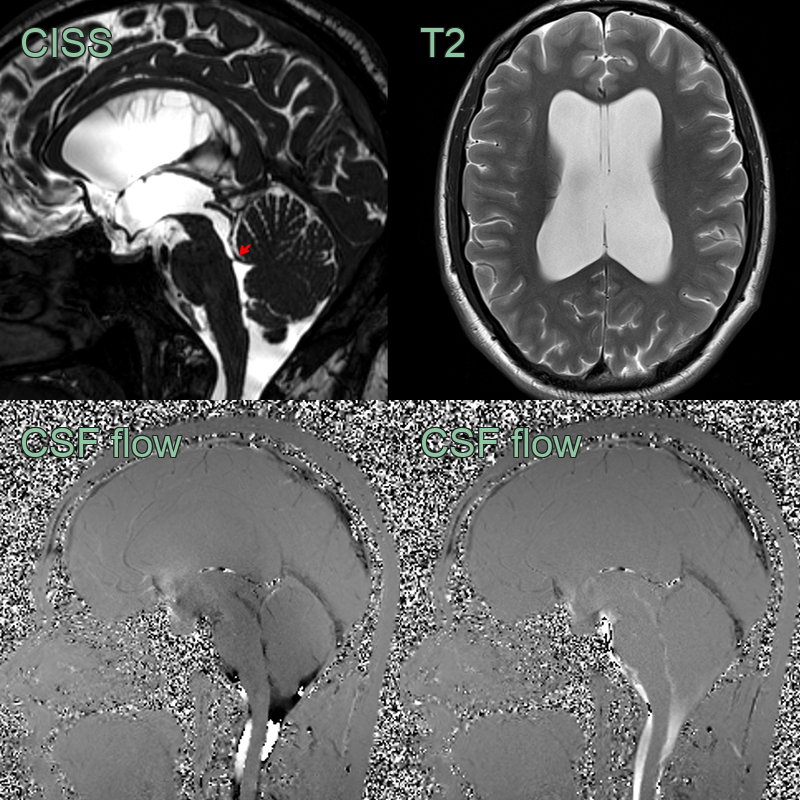
- A 40-year-old patient had an MRI scan due to chronic but increasing headaches.
- MRI showed a focal filling defect in the inferior Sylvian aqueduct.
- CSF flow studies showed normal biphasic flow indicating a stenosis rather than an obstruction.
Treatment¶
- Medical management:
- Acetazolamide to reduce CSF production (temporary measure)
- Treatment of underlying causes (e.g., infections, tumours)
- Surgical interventions:
- Endoscopic third ventriculostomy (ETV):
- First-line treatment in many cases
- Creates alternative CSF pathway
- Ventriculoperitoneal (VP) shunt:
- Alternative to ETV or in cases of ETV failure
- Aqueductoplasty:
- Endoscopic procedure to restore aqueduct patency
- Follow-up:
- Regular neuroimaging to assess ventricular size
- Neurological and developmental assessments
- Shunt function monitoring (if applicable)
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Aqueductal web | Thin membrane visible on high-resolution MRI |
| Tectal glioma | Presence of a mass lesion in the tectal plate on MRI |
| Pineal region tumour | Visible mass in the pineal region on imaging studies |
| Dandy-Walker malformation | Cystic dilatation of 4th ventricle and cerebellar vermis hypoplasia |
| Chiari malformation | Downward displacement of cerebellar tonsils on MRI |
| Benign intracranial hypertension | Normal or small ventricles on imaging |
| Communicating hydrocephalus | Enlargement of all ventricles without obvious obstruction |
| Arachnoid cyst | Well-defined, extra-axial CSF-density lesion on CT/MRI |
| Vein of Galen malformation | Dilated vein of Galen visible on angiography or MRI |
| Craniosynostosis | Premature fusion of cranial sutures on CT |