Toxoplasmosis¶
Summary
- Parasitic infection caused by Toxoplasma gondii
- Typically asymptomatic in immunocompetent individuals
- Can cause severe complications in immunocompromised patients and congenital infections
Pathophysiology¶
- Caused by the protozoan parasite Toxoplasma gondii
- Transmission:
- Ingestion of undercooked meat containing tissue cysts
- Consumption of food or water contaminated with oocysts shed in cat feces
- Transplacental transmission from mother to fetus
- Life cycle:
- Definitive hosts: Felids (domestic and wild cats)
- Intermediate hosts: Warm-blooded animals, including humans
- Tachyzoites invade host cells and replicate, leading to cell lysis and spread
Demographics¶
- Worldwide distribution
- Seroprevalence:
- Varies by geographic region and cultural practices
- Estimated 30-50% of global population infected
- Higher risk groups:
- Immunocompromised individuals (HIV/AIDS, organ transplant recipients)
- Pregnant women
- Individuals with frequent exposure to cats or raw meat
Diagnosis¶
- Serology:
- IgG and IgM antibodies
- IgG avidity test to determine timing of infection
- PCR:
- Detection of T. gondii DNA in blood, cerebrospinal fluid, or amniotic fluid
- Histopathology:
- Tissue biopsy with characteristic findings
- Clinical presentation:
- Often asymptomatic in immunocompetent individuals
- Flu-like symptoms in acute infection
- Severe manifestations in immunocompromised patients (encephalitis, pneumonitis)
- Congenital toxoplasmosis: hydrocephalus, intracranial calcifications, chorioretinitis
Imaging¶
- Central Nervous System:
- CT:
- Multiple ring-enhancing lesions
- Cerebral oedema
- Hydrocephalus (in congenital cases)
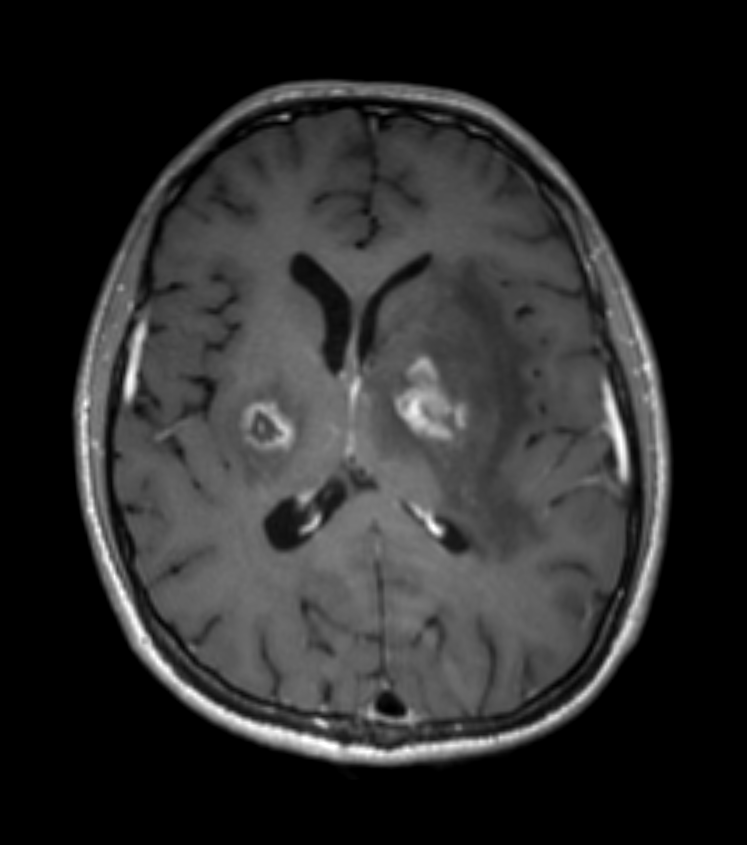
- MRI:
- T1: Hypointense lesions
- T2: Hyperintense lesions with surrounding oedema
- Post-contrast: Ring-enhancing lesions
- Ocular:
- Ultrasound: Hyperechoic foci in vitreous
- Fluorescein angiography: Active chorioretinitis
- Congenital:
- Intracranial calcifications
- Ventriculomegaly
- Cortical atrophy
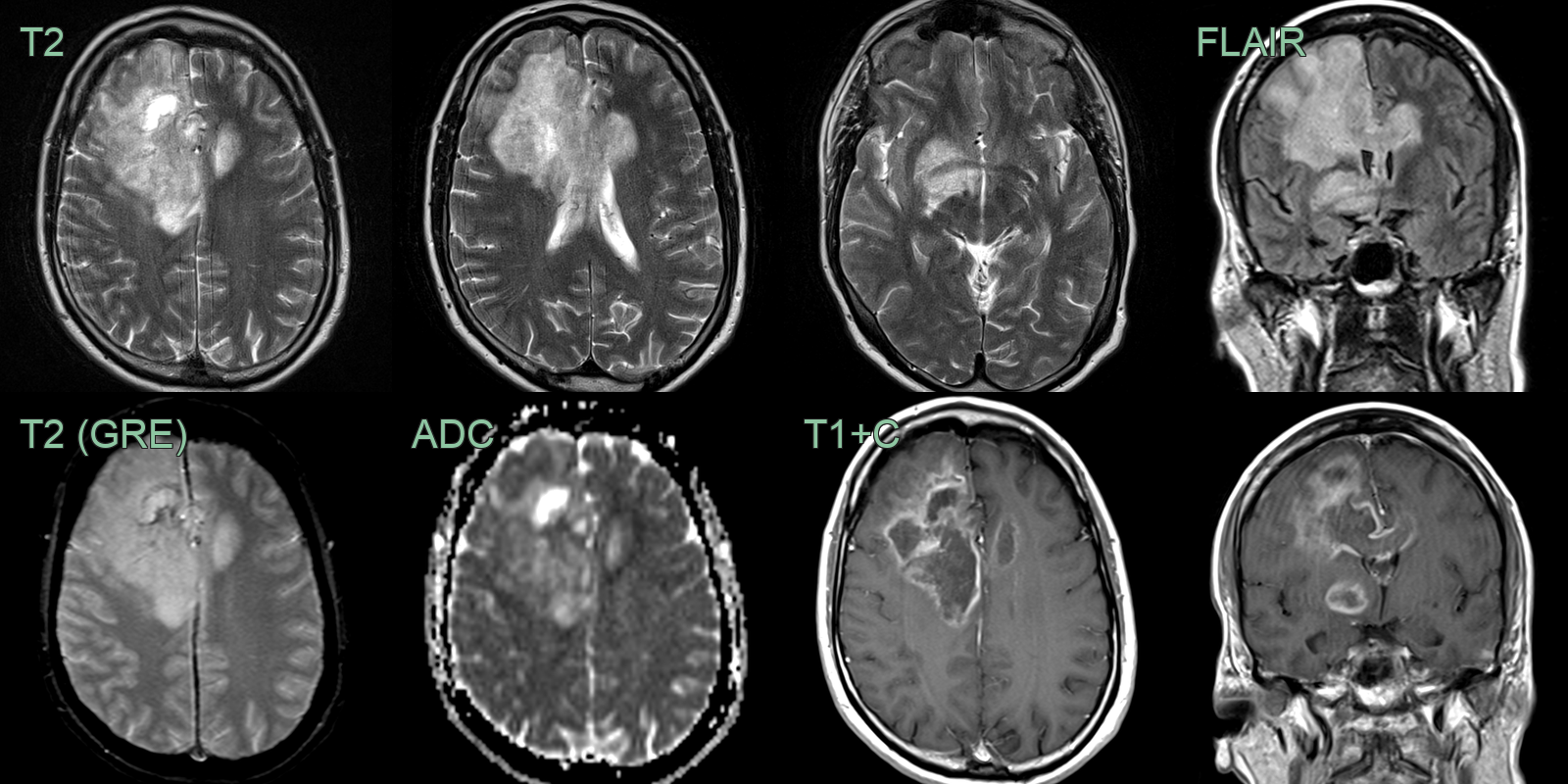
- 50-year-old patient presented with a new diagnosis of HIV with a CD4 count of 50.
- MRI showed multple large right frontal lesions with peripheral enhancement, diffusion restriction and petechial haemorrhage.
- With differential diagnosis of lymphoma, the diagnosis of toxoplasmosis was made after a right frontal biopsy.
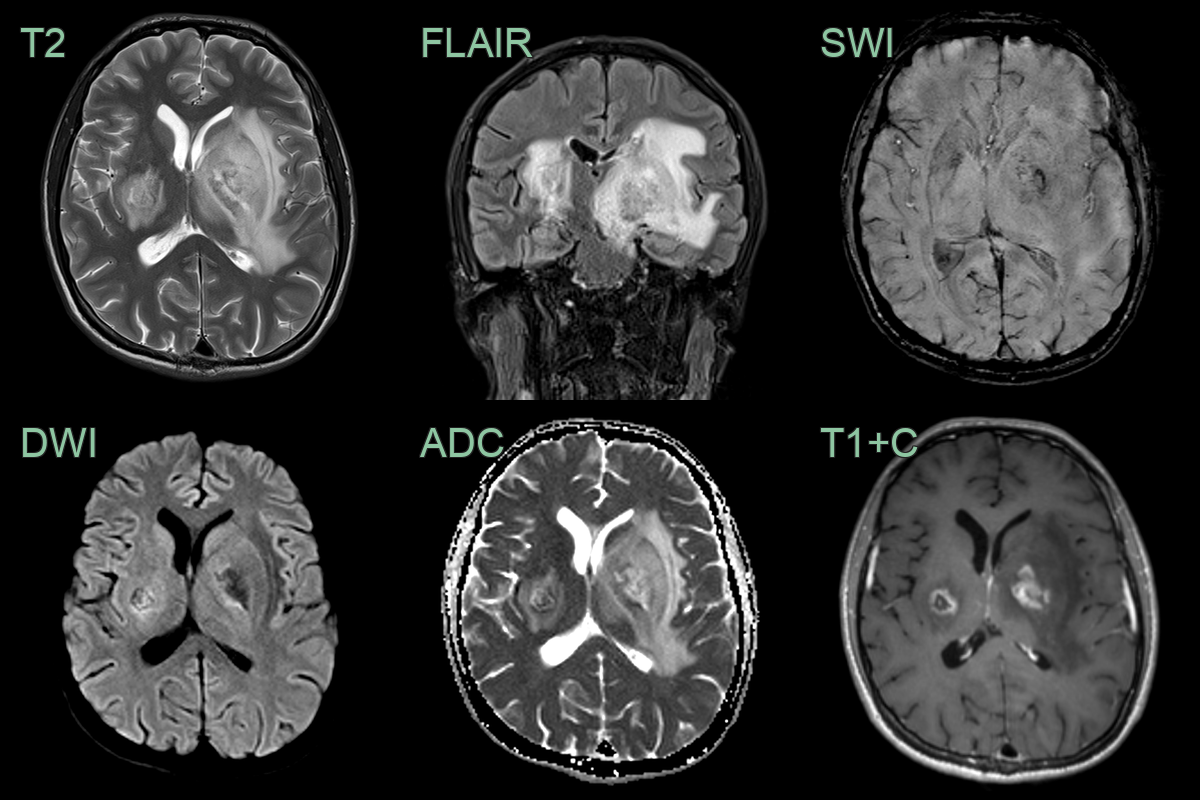
- Patient with a new diagnosis of HIV (CD4 count of <50) presented with headache and right sided weakness.
- MRI showed many peripherally/irregularly enhancing lesions in both cerebral hemispheres and the cerebellum.
- Toxoplasma serology was positive.
Treatment¶
- Immunocompetent individuals:
- Often self-limiting, no treatment required for mild cases
- Immunocompromised patients and severe cases:
- Pyrimethamine + sulfadiazine + leucovorin
- Alternative: Trimethoprim-sulfamethoxazole
- Pregnant women:
- Spiramycin (to prevent fetal transmission)
- Pyrimethamine + sulfadiazine + leucovorin (if fetal infection confirmed)
- Congenital toxoplasmosis:
- Pyrimethamine + sulfadiazine + leucovorin for 12 months
- Ocular toxoplasmosis:
- Antiparasitic therapy + corticosteroids
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| HIV encephalopathy | Lack of focal lesions on imaging; diffuse white matter changes |
| Primary CNS lymphoma | Single lesion more common; intense contrast enhancement |
| Brain abscess | Ring-enhancing lesion with restricted diffusion on MRI |
| Neurocysticercosis | Multiple small cystic lesions; calcifications in chronic stage |
| Tuberculoma | Thick-walled lesions; basal meningeal enhancement |
| Progressive multifocal leukoencephalopathy (PML) | No contrast enhancement; subcortical white matter involvement |
| Cryptococcosis | Gelatinous pseudocysts in basal ganglia and perivascular spaces; T2 hyperintense cystic lesions with minimal enhancement |
| Cerebral metastases | Multiple lesions at grey-white matter junction; ring or nodular enhancement; surrounding vasogenic oedema |
| Acute disseminated encephalomyelitis (ADEM) | Bilateral, large confluent white matter lesions; may involve basal ganglia; no ring enhancement |
| Neurosarcoidosis | Leptomeningeal enhancement; hilar lymphadenopathy on chest imaging |