Trigeminal Artery¶
Summary
- Persistent trigeminal artery (PTA) is the most common persistent carotid-basilar anastomosis
- Embryonic connection between the cavernous portion of the internal carotid artery and the basilar artery
- Usually asymptomatic but can be associated with various neurological symptoms and vascular anomalies
Pathophysiology¶
- Embryologically, the trigeminal artery develops around the 3rd week of gestation
- Normally regresses by the 7th-8th week of gestation
- Persistence occurs when the artery fails to regress and remains patent
- Two main types:
- Lateral (petrosal) variant: More common, courses lateral to the dorsum sellae
- Medial (sphenoidal) variant: Less common, courses medial to the dorsum sellae
Demographics¶
- Incidence: 0.1-0.6% of cerebral angiograms
- No significant gender predilection
- Can be found in all age groups, but more commonly diagnosed in adults
Diagnosis¶
- Often an incidental finding on imaging studies
- Clinical presentation:
- Usually asymptomatic
- May present with:
- Trigeminal neuralgia
- Oculomotor palsy
- Abducens nerve palsy
- Cerebrovascular insufficiency
Imaging¶
- Angiography (DSA, CTA, or MRA):
- Gold standard for diagnosis
- Demonstrates direct connection between internal carotid artery and basilar artery
- CT:
- May show a rounded or tubular structure in the prepontine cistern
- Calcifications may be present
- MRI:
- T1 and T2-weighted images: Flow void in the prepontine cistern
- MRA: Clearly demonstrates the persistent trigeminal artery
- Associated findings:
- Hypoplasia of the basilar artery proximal to the PTA junction
- Absence or hypoplasia of the posterior communicating arteries
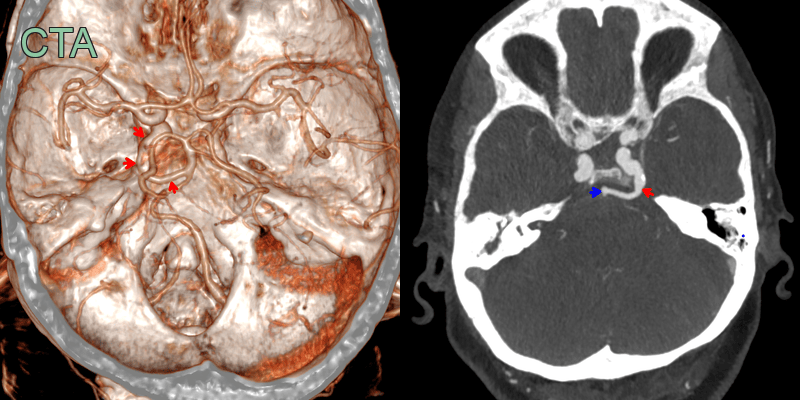
- Incidental finding of a trigeminal artery (red arrow) forming and anastomosis between the cavernous ICA and the basilar artery (blue arrow).
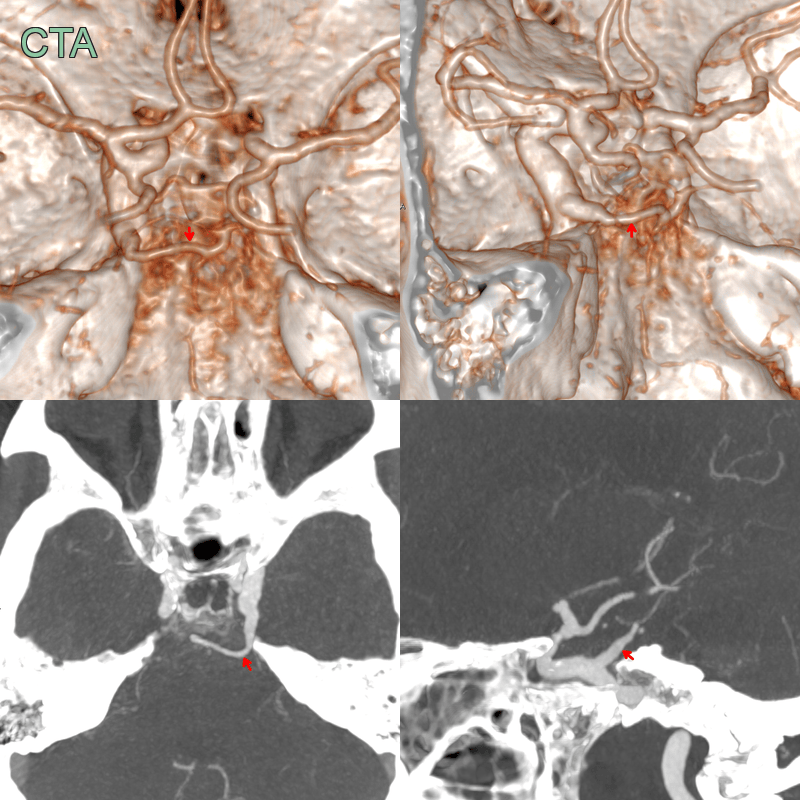
- Incidential finding of an anastomosis between the cavernous left ICA and the posterior circulation (red arrow).
- The vertebrobasilar system was hypoplastic.
Treatment¶
- Generally, no treatment required for asymptomatic cases
- Management focuses on associated conditions:
- Aneurysms: Endovascular coiling or surgical clipping
- Trigeminal neuralgia: Medical management or microvascular decompression
- Cerebrovascular insufficiency: Antiplatelet therapy or revascularization procedures
- Endovascular treatment may be considered in symptomatic cases:
- Occlusion of the PTA using detachable balloons or coils
- Stent-assisted coiling for associated aneurysms
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Persistent Hypoglossal Artery | Arises from cervical internal carotid artery and enters skull through hypoglossal canal |
| Persistent Proatlantal Artery | Connects vertebral artery to external carotid artery |
| Persistent Otic Artery | Passes through internal acoustic meatus |
| Aberrant Internal Carotid Artery | Courses through middle ear cavity |
| Basilar Artery Fenestration | Involves duplication of a segment of the basilar artery |
| Arteriovenous Malformation | Abnormal tangle of blood vessels with direct arterial-venous shunting |
| Aneurysm | Focal dilatation of an artery, typically saccular or fusiform in shape |
| Cavernous Sinus Fistula | Abnormal communication between carotid artery and cavernous sinus |
| Moyamoya Disease | Progressive stenosis of distal internal carotid arteries with collateral vessel formation |
| Basilar Artery Hypoplasia | Underdevelopment of the basilar artery, often associated with persistent fetal circulation |