Trigeminal Schwannoma¶
Summary
- Rare benign tumour arising from Schwann cells of the trigeminal nerve
- Presents with facial pain, numbness, or weakness in trigeminal nerve distribution
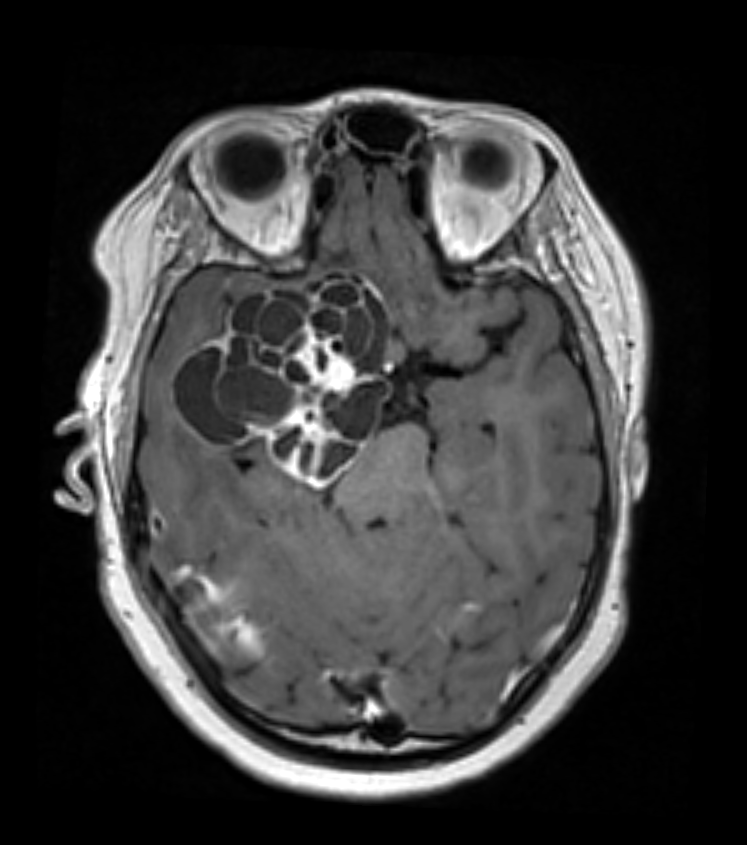
- Imaging shows a dumbbell-shaped mass in the middle cranial fossa and/or posterior fossa
Pathophysiology¶
- Originates from Schwann cells of the trigeminal nerve sheath
- Most commonly arises from the gasserian ganglion in the middle cranial fossa
- Can extend into the posterior fossa through Meckel's cave
- May involve one or more divisions of the trigeminal nerve
Demographics¶
- Accounts for 0.07-0.36% of all intracranial tumours
- Peak incidence in 4th to 5th decades of life
- No significant gender predilection
- Rare association with neurofibromatosis type 2 (NF2)
Diagnosis¶
- Clinical presentation:
- Facial pain or numbness in trigeminal nerve distribution
- Facial weakness or paralysis
- Headache
- Hearing loss or tinnitus (if involving the cerebellopontine angle)
- Physical examination:
- Decreased sensation in trigeminal nerve distribution
- Weakness of masticatory muscles
- Corneal reflex abnormalities
Imaging¶
- MRI:
- T1-weighted: iso- to hypointense
- T2-weighted: hyperintense
- Contrast-enhanced T1: heterogeneous enhancement
- Characteristic dumbbell shape extending through Meckel's cave
- CT:
- Isodense to brain parenchyma
- Bone window: widening of foramen ovale or rotundum
- Angiography:
- May show tumour blush or displacement of adjacent vessels
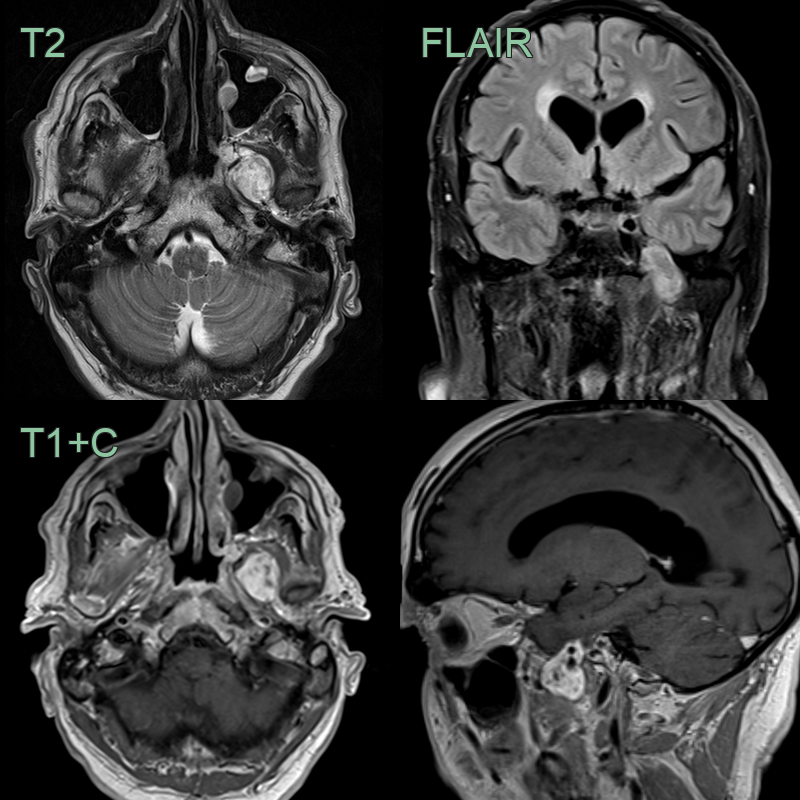
- An incidental hetergeneously enhancing lesion was traversing an expanded left foramen ovale.
- As the lesion was incidental and there was no growth over 3 years, no treatment was planned.
- The putative diagnosis was a V3 trigeminal schwannoma.
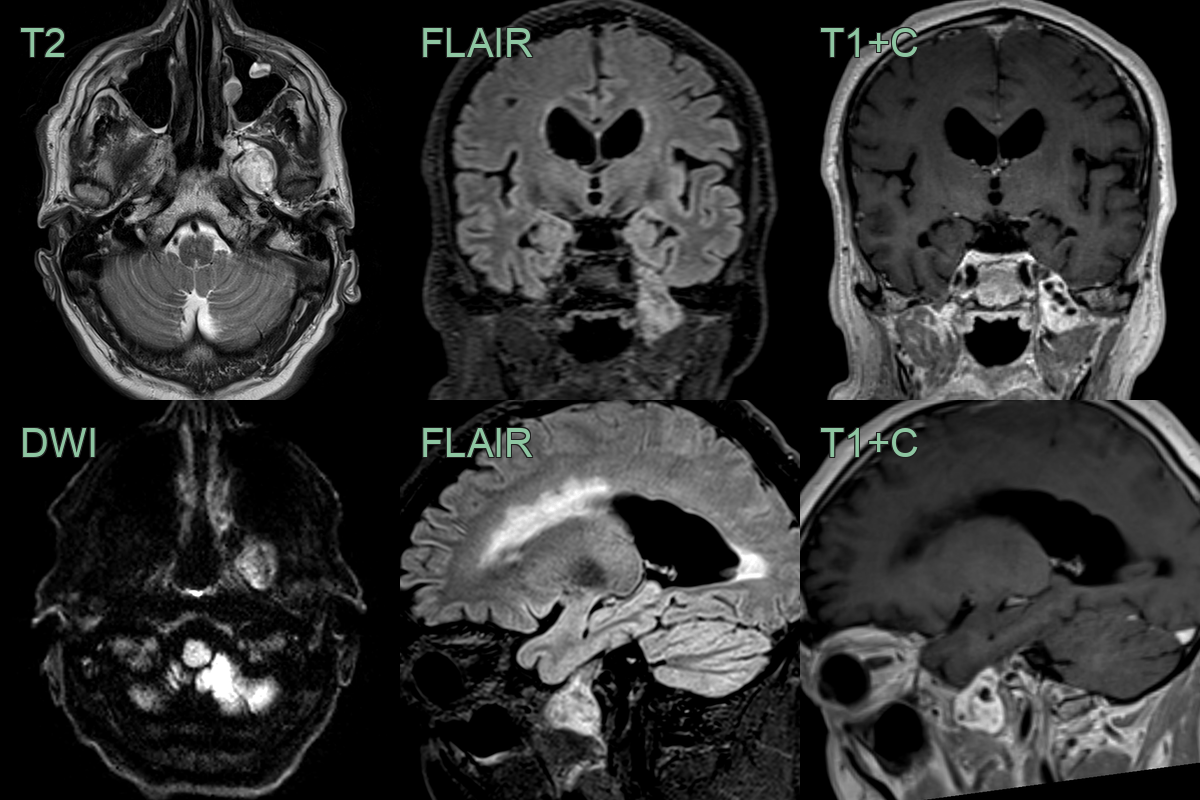
- An incidental lesion was found expanding the foramen ovale on the left.
- The lesion was avidly enhacning with small cystic components.
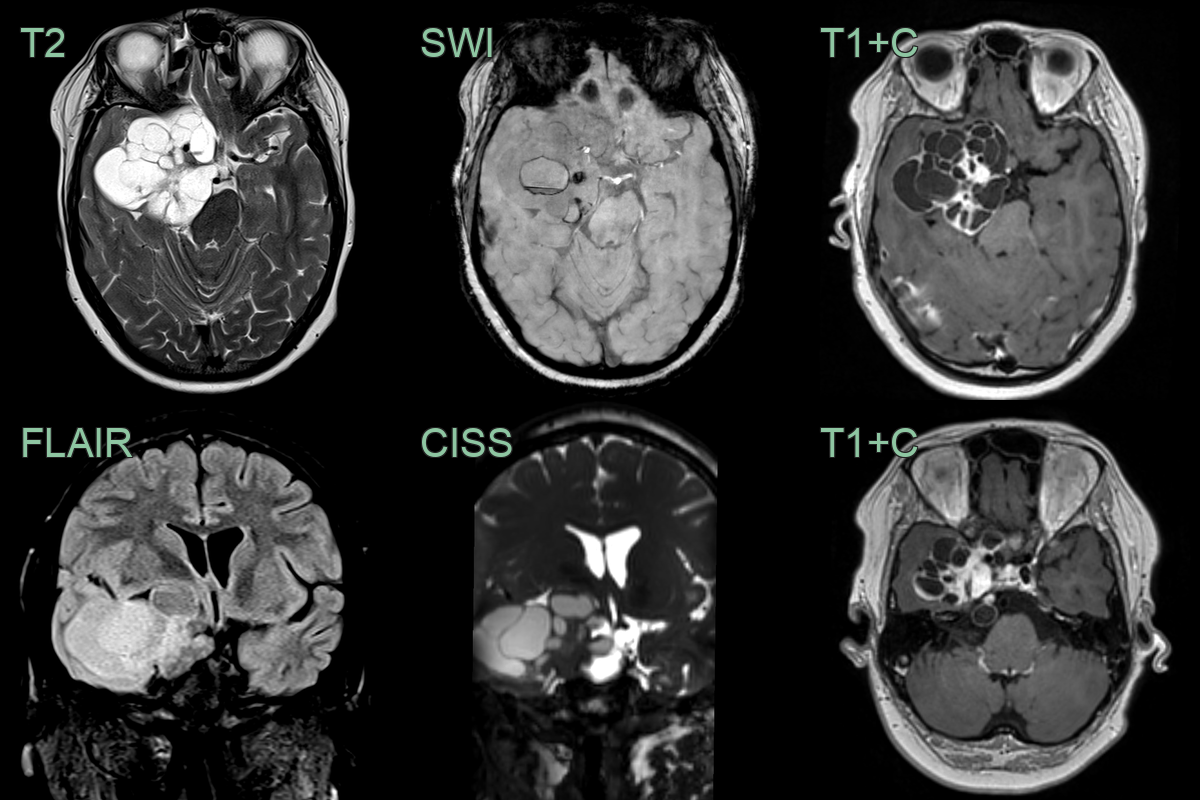
- A 25-year-old patient presented with right sided facial numbness and diplopia.
- MRI showed a solid-cystic partially enhancing lesion that involved the cavernous sinus.
- A schwannoma was confirmed following resection.
Treatment¶
- Surgical resection:
- Primary treatment modality
- Approach depends on tumour location and extent
- Options include middle fossa, retrosigmoid, or combined approaches
- Stereotactic radiosurgery:
- Alternative for small tumours or residual disease
- Useful in patients unsuitable for surgery
- Follow-up:
- Regular MRI surveillance to monitor for recurrence
- Long-term follow-up recommended due to potential for late recurrence
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Meningioma | Typically has a dural tail on MRI; schwannomas do not |
| Acoustic neuroma | Primarily affects the vestibulocochlear nerve; trigeminal schwannomas affect the trigeminal nerve |
| Epidermoid cyst | Demonstrates restricted diffusion on DWI; schwannomas do not |
| Metastasis | Often multiple lesions; schwannomas are typically solitary |
| Chordoma | Occurs in the clivus; trigeminal schwannomas are along the course of the trigeminal nerve |
| Pituitary adenoma | Centered in the sella turcica; trigeminal schwannomas are not |
| Aneurysm | Demonstrates flow voids on MRI; solid enhancement in schwannomas |
| Glioma | Infiltrative appearance; schwannomas are well-circumscribed |
| Hemangiopericytoma | Typically has a multilobulated appearance; schwannomas are more uniform |
| Chondrosarcoma | Often has calcifications; not typical in schwannomas |