Tumefactive Demyelination¶
Summary
- Rare form of demyelinating disease characterised by large (>2 cm) lesions mimicking brain tumours
- Presents with acute or subacute neurological deficits, headache, and seizures
- MRI shows large, solitary or multiple lesions with variable enhancement and oedema
Pathophysiology¶
- Exact mechanism unclear, but involves immune-mediated destruction of myelin
- May represent a severe variant of multiple sclerosis or other demyelinating disorders
- Characterised by large areas of myelin loss with relative axonal preservation
- Inflammatory infiltrates consist of T-cells, macrophages, and occasional B-cells
Demographics¶
- Typically affects young to middle-aged adults (20-45 years)
- Slight female predominance (1.2:1 female to male ratio)
- Rare in children and older adults
- No clear ethnic or geographic predilection
Diagnosis¶
- Clinical presentation:
- Acute or subacute onset of neurological deficits
- Headache, seizures, cognitive changes
- Focal neurological signs depending on lesion location
- Laboratory findings:
- CSF analysis may show mild pleocytosis and elevated protein
- Oligoclonal bands may be present in some cases
- Differential diagnosis:
- Primary brain tumours (e.g., gliomas)
- Metastases
- Abscess
- Lymphoma
Imaging¶
- MRI:
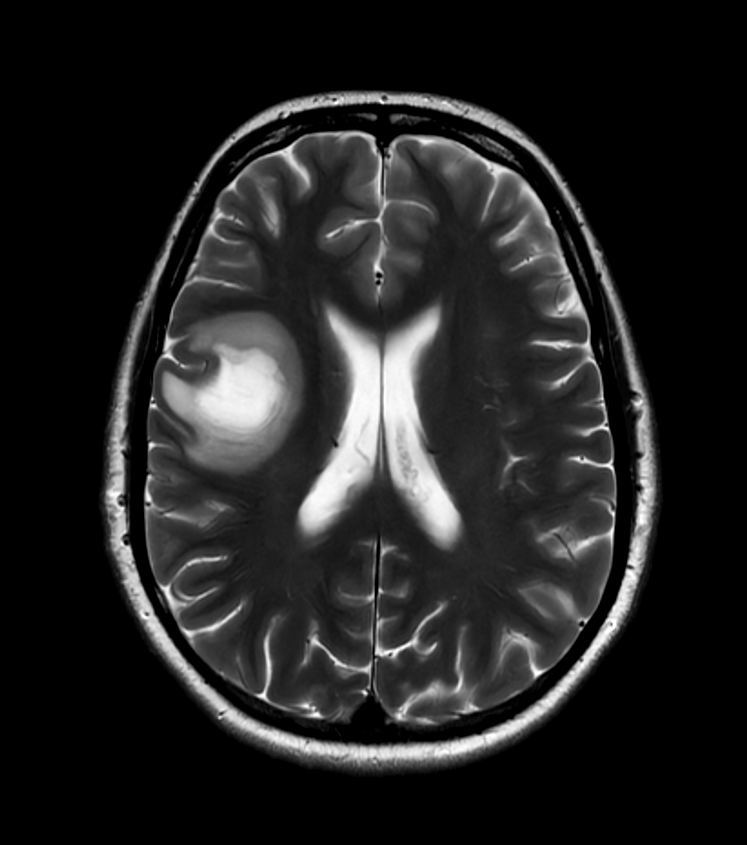
- Large (>2 cm) lesions, often solitary but can be multiple
- T2/FLAIR: Hyperintense with surrounding oedema
- T1: Hypointense to isointense
- Contrast enhancement: Variable, can be ring-like, nodular, or homogeneous
- Incomplete ring enhancement with open side facing cortex ("open-ring sign")
- Advanced MRI techniques:
- MR spectroscopy: Elevated choline, reduced N-acetylaspartate, presence of lactate/lipid peaks
- Diffusion-weighted imaging: Variable findings, often increased diffusivity
- Perfusion imaging: Generally decreased perfusion compared to neoplasms
- CT:
- Hypodense lesions with variable enhancement
- Less sensitive than MRI for detecting and characterising lesions
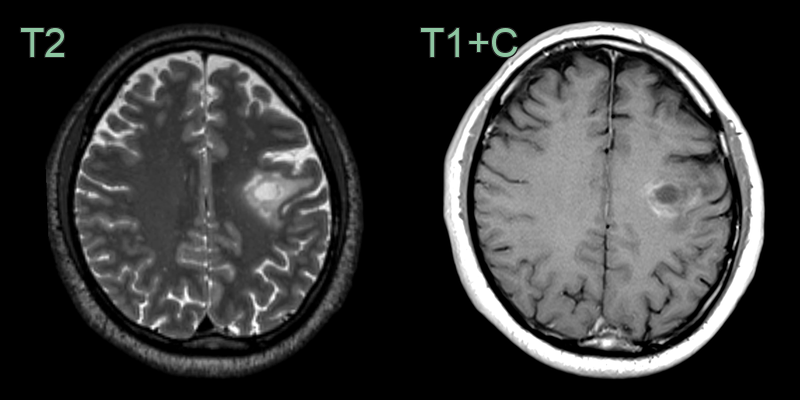
- A 40-year-old patient presented with expressive dysphasia.
- MRI showed a peripherally enhancing lesion in the left posterior frontal lobe.
- Biopsy revealed inflammatory demyelination.
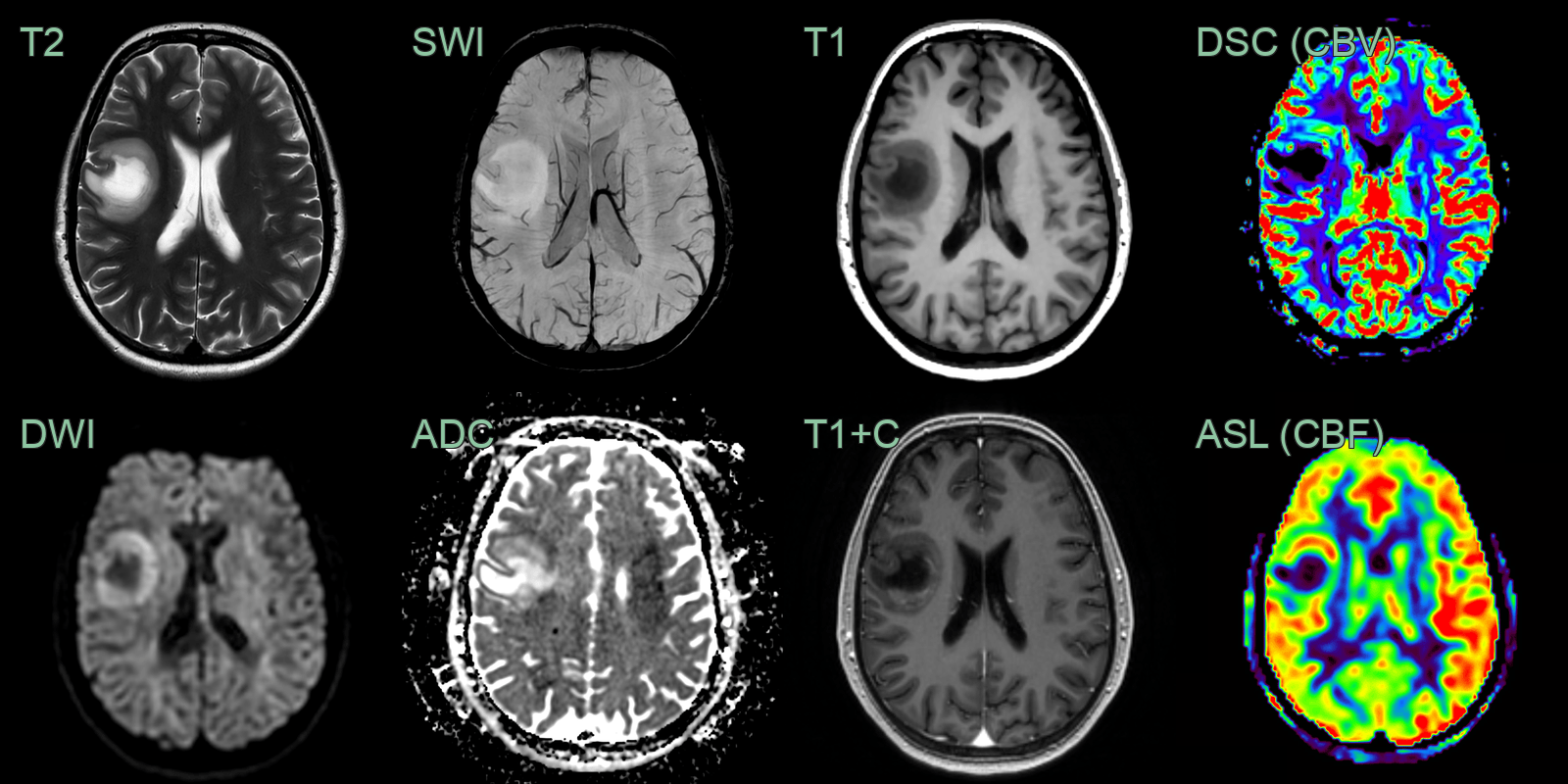
- A 30-year-old patient presented with a left-sided facial droop and speech disturbance.
- MRI showed a T2-hyperintense lesion in the right posterior frontal lobe with a rim of enhancement and diffusion restriction.
- DSC and ASL perfusion showed elevated CBV and CBF peripherally (corresponding to the diffusion restriction).
- Biopsy confirmed inflammatory demyelination.
Treatment¶
- Corticosteroids:
- High-dose intravenous methylprednisolone (1g daily for 3-5 days)
- Followed by oral prednisone taper
- Plasmapheresis:
- Consider in cases refractory to corticosteroids
- Immunomodulatory therapies:
- May be considered for long-term management, especially if associated with multiple sclerosis
- Symptomatic management:
- Antiepileptic drugs for seizures
- Pain management as needed
- Follow-up imaging:
- Serial MRI to monitor treatment response and exclude alternative diagnoses
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Glioblastoma | Tumefactive demyelination typically has incomplete ring enhancement, while glioblastoma often shows complete ring enhancement |
| Primary CNS Lymphoma | Tumefactive demyelination usually has less mass effect and oedema compared to lymphoma |
| Brain Abscess | Tumefactive demyelination lacks diffusion restriction in the centre, which is typically seen in abscesses |
| Metastatic Brain Tumour | Tumefactive demyelination often has a single lesion, while metastases are usually multiple |
| Acute Disseminated Encephalomyelitis (ADEM) | Bilateral, large confluent T2 lesions involving grey and white matter; incomplete ring enhancement; may involve basal ganglia and thalami |
| Subacute Infarct | Tumefactive demyelination does not follow a vascular territory, unlike infarcts |
| Progressive Multifocal Leukoencephalopathy (PML) | Tumefactive demyelination usually has more mass effect than PML lesions |
| Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) | Tumefactive demyelination lacks the characteristic involvement of anterior temporal lobes and external capsules seen in CADASIL |
| Neurosarcoidosis | Tumefactive demyelination typically lacks leptomeningeal enhancement, which is common in neurosarcoidosis |
| Cerebral Vasculitis | Tumefactive demyelination usually presents as a single large lesion, while vasculitis often causes multiple smaller lesions |