Tumefactive Perivascular Spaces¶
Summary
- Tumefactive perivascular spaces (TPVS) are abnormally enlarged perivascular spaces that can mimic cystic neoplasms
- Typically found in the basal ganglia, centrum semiovale, and midbrain
- Characterised by well-defined, round or oval cystic lesions following CSF signal on all sequences
Pathophysiology¶
- Perivascular spaces (PVS) are extensions of the subarachnoid space that surround penetrating arteries
- TPVS occur when these spaces become abnormally enlarged, potentially due to:
- Obstruction of CSF flow
- Increased permeability of vessel walls
- Impaired drainage of interstitial fluid
Demographics¶
- More common in elderly patients
- No significant gender predilection
- Associated with:
- Hypertension
- Dementia
- Small vessel disease
- Mucopolysaccharidoses
Diagnosis¶
- Often an incidental finding on neuroimaging
- Clinical presentation:
- Usually asymptomatic
- Rarely, may cause mass effect leading to headaches or focal neurological deficits
- Differential diagnosis:
- Cystic neoplasms
- Lacunar infarcts
- Cryptococcosis
- Neurocysticercosis
Imaging¶
- CT:
- Well-defined, round or oval hypodense lesions
- No enhancement with contrast
- MRI:
- T1: Hypointense
- T2/FLAIR: Hyperintense, following CSF signal
- DWI: No restricted diffusion
- No enhancement on post-contrast T1
- Key features:
- Cluster of cystic lesions
- No surrounding oedema
- No mass effect
- Typically bilateral and symmetrical
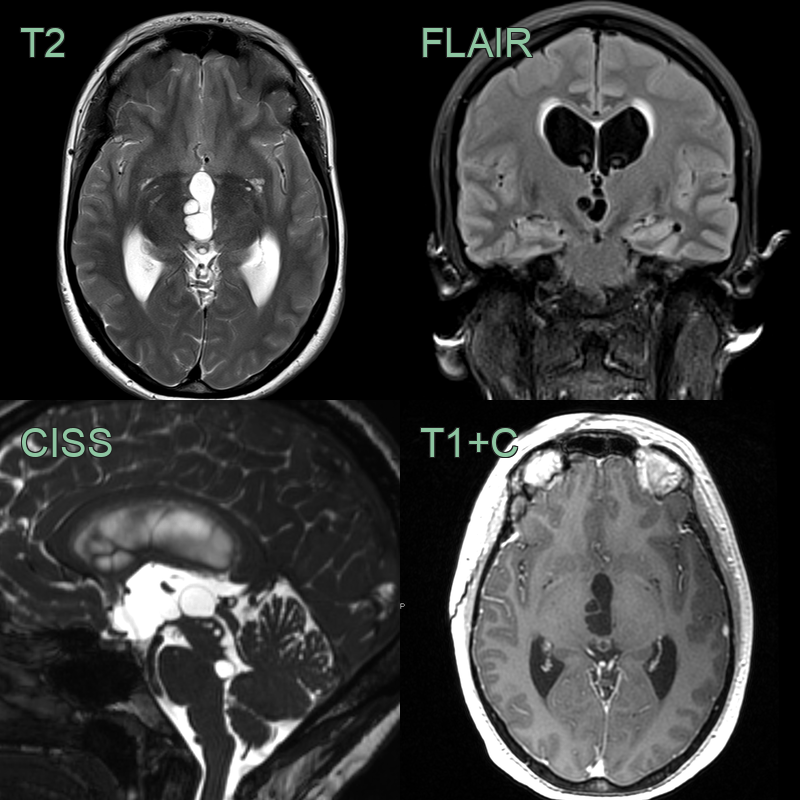
- 40-year-old patient presenting with headache.
- There was chronic ventriculomegaly although the periventricular oedema had increased since imaging 1 year prior.
- CSF outflow through the sylvian aqueduct was impaired by cystic lesions in the right paramedian thalamus and in the midbrain.
- The cysts had not changed in 1 year and there was no soft tissue component or pathological enhancement to indicate a neoplasm.
Treatment¶
- No specific treatment required for asymptomatic TPVS
- Management focuses on underlying conditions (e.g., hypertension, small vessel disease)
- In rare cases of symptomatic TPVS:
- Surgical decompression may be considered
- CSF diversion procedures (e.g., ventriculoperitoneal shunt) for hydrocephalus
- Follow-up imaging to monitor for stability and exclude neoplastic processes
Differential diagnosis¶
| Differential Diagnosis | Differentiating Feature |
|---|---|
| Low-grade glioma | Enhances with contrast, shows mass effect |
| Multiple sclerosis | Ovoid lesions, periventricular distribution |
| Lacunar infarcts | Irregular borders, restricted diffusion on DWI |
| Cryptococcosis | Gelatinous pseudocysts in basal ganglia showing T2 hyperintensity with restricted diffusion; may show enhancement |
| Neurocysticercosis | Cystic lesions with enhancing scolex; calcifications in chronic stage on CT |
| Metastases | Multiple lesions with ring or nodular enhancement and surrounding vasogenic oedema |
| Mucopolysaccharidosis | Diffuse white matter T2 changes; enlarged perivascular spaces similar in appearance but more diffuse |
| Small vessel disease | Irregular borders, associated white matter hyperintensities |
| Virchow-Robin spaces | Smaller size, typically <3mm |
| Arachnoid cysts | Extra-axial location, CSF signal on all sequences |