Vascular Dementia¶
Summary
- Vascular dementia is cognitive impairment caused by cerebrovascular disease
- Characterised by stepwise decline in cognitive function
- Imaging shows multiple infarcts, white matter changes, or strategic single infarcts
Pathophysiology¶
- Caused by reduced blood flow to the brain due to:
- Multiple small vessel infarcts
- Large vessel occlusions
- Chronic hypoperfusion
- Results in neuronal death and cognitive decline
- Vascular risk factors contribute to endothelial dysfunction and blood-brain barrier disruption
Demographics¶
- Second most common cause of dementia after Alzheimer's disease
- Prevalence increases with age:
- 1-4% in individuals 65-69 years
- 14-16% in those over 80 years
- Higher incidence in men and individuals of African or Asian descent
Diagnosis¶
- Clinical presentation:
- Stepwise cognitive decline
- Focal neurological signs
- Gait disturbances
- Urinary incontinence
- Neuropsychological testing:
- Executive function deficits
- Slowed processing speed
- Impaired attention and concentration
- Diagnostic criteria:
- Evidence of cognitive decline
- Presence of cerebrovascular disease
- Temporal relationship between vascular events and cognitive decline
Imaging¶
- CT findings:
- Multiple lacunar infarcts
- Cortical infarcts
- White matter hypodensities
- MRI findings:
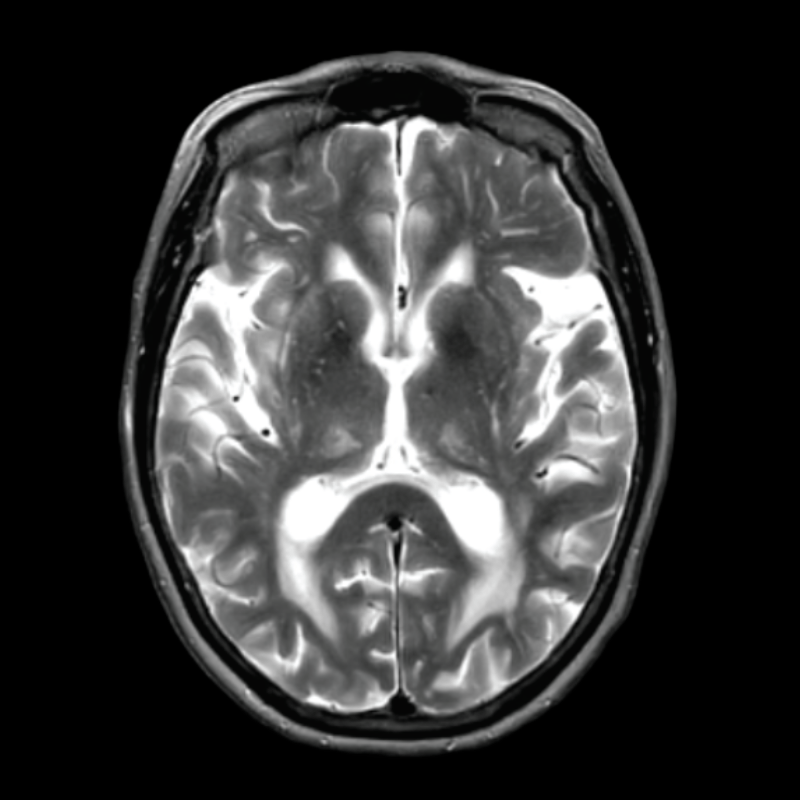
- T2/FLAIR hyperintensities in white matter and deep gray nuclei
- Microbleeds on susceptibility-weighted imaging
- Strategic infarcts (e.g., thalamus, angular gyrus)
- Advanced techniques:
- DTI: reduced fractional anisotropy in white matter tracts
- Perfusion imaging: areas of hypoperfusion
- MR spectroscopy: reduced N-acetylaspartate/creatine ratio
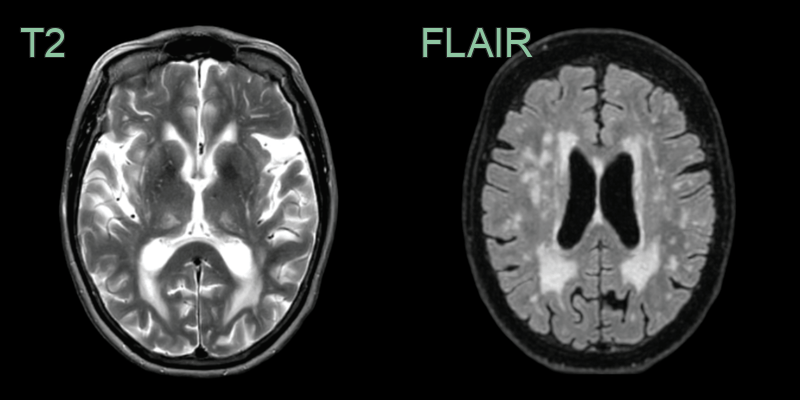
- 75-year-old patient with many cardiovascular risk factors presented with impaired memory and depression.
- There was a severe burden of small vessel disease that invovled the dorsal thalami bilaterally.
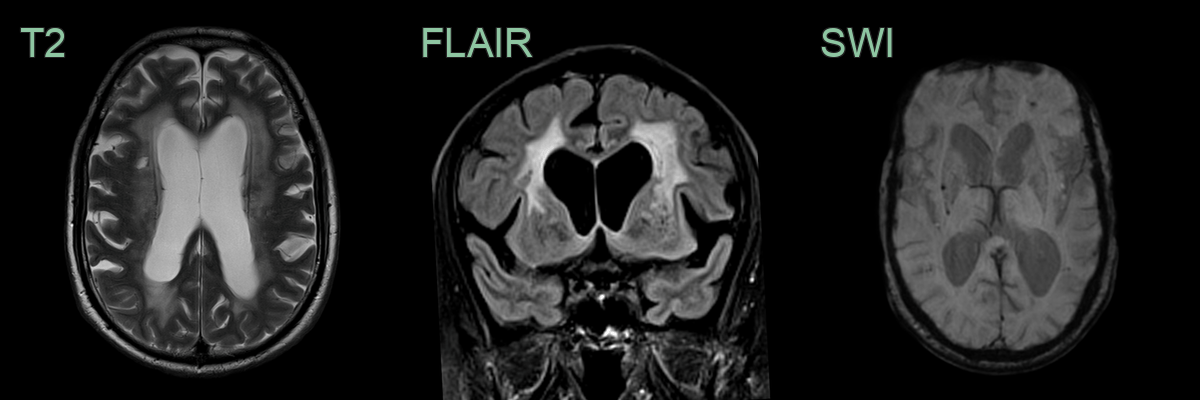
- A 70-year-old patient with hypertension (now controlled on 3 agents) presented with cognitive impairment affecting mutliple domains.
- MRI showed Fazekas grade 3 small vessel disease and multiple deep microhaemorrhages.
Treatment¶
- Management of vascular risk factors:
- Hypertension control
- Diabetes management
- Smoking cessation
- Lipid-lowering therapy
- Antiplatelet therapy for secondary stroke prevention
- Cognitive rehabilitation and occupational therapy
- Cholinesterase inhibitors may provide modest cognitive benefit
- No disease-modifying treatments currently available
Differential diagnosis¶
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Alzheimer's Disease | Hippocampal and entorhinal atrophy on MRI; posterior parietal and precuneus hypometabolism on FDG-PET; lesser burden of white matter hyperintensities and lacunar infarcts |
| Lewy Body Dementia | Occipital hypometabolism on FDG-PET; less prominent white matter disease; midbrain atrophy |
| Frontotemporal dementia | Frontal and anterior temporal atrophy without significant white matter hyperintensities or lacunar infarcts |
| Creutzfeldt-Jakob disease | Cortical ribbon and basal ganglia DWI restriction; pulvinar sign on T2; rapid cortical atrophy on follow-up |
| CADASIL | Anterior temporal pole and external capsule FLAIR hyperintensity; subcortical lacunar infarcts; microbleeds |