Vasculitis¶
Summary
- Vasculitis is inflammation of blood vessel walls, leading to organ damage
- Classified by vessel size affected and underlying aetiology (e.g. autoimmune, infectious)
- Imaging findings vary but often show vessel wall thickening, stenosis, or aneurysms
Pathophysiology¶
- Inflammation of blood vessel walls leads to:
- Vessel wall thickening and narrowing of lumen
- Weakening of vessel walls, potentially causing aneurysms
- Tissue ischaemia due to compromised blood flow
- Vessel occlusion from thrombosis
- Immune-mediated mechanisms often involved:
- Antineutrophil cytoplasmic antibodies (ANCA)
- Immune complex deposition
- T-cell-mediated inflammation
Demographics¶
- Incidence varies by specific type of vasculitis
- Generally affects all age groups, but some types more common in certain demographics:
- Giant cell arteritis: typically affects those >50 years
- Kawasaki disease: primarily affects children <5 years
- Takayasu arteritis: more common in young women
- Some types show geographical or ethnic predilections:
- Behçet's disease: more prevalent along the ancient Silk Road
Diagnosis¶
- Clinical presentation varies widely depending on affected vessels and organs
- Laboratory tests:
- Elevated inflammatory markers (ESR, CRP)
- ANCA testing for certain types (e.g. granulomatosis with polyangiitis)
- Complement levels
- Tissue biopsy: often considered the gold standard for diagnosis
- Imaging plays a crucial role in diagnosis and monitoring
Imaging¶
- Modalities used:
- Ultrasound: for superficial vessels and temporal arteries
- CT angiography: excellent for medium and large vessel evaluation
- MR angiography: useful for follow-up and reducing radiation exposure
- PET-CT: can detect early inflammatory changes and assess disease activity
- Common findings:
- Vessel wall thickening and enhancement
- Luminal narrowing or occlusion
- Aneurysm formation
- Vessel wall calcification in chronic cases
- Surrounding soft tissue inflammation
- Specific patterns:
- Large vessel vasculitis: aorta and major branch involvement
- Medium vessel vasculitis: renal, hepatic, and mesenteric artery involvement
- Small vessel vasculitis: often manifests as end-organ damage
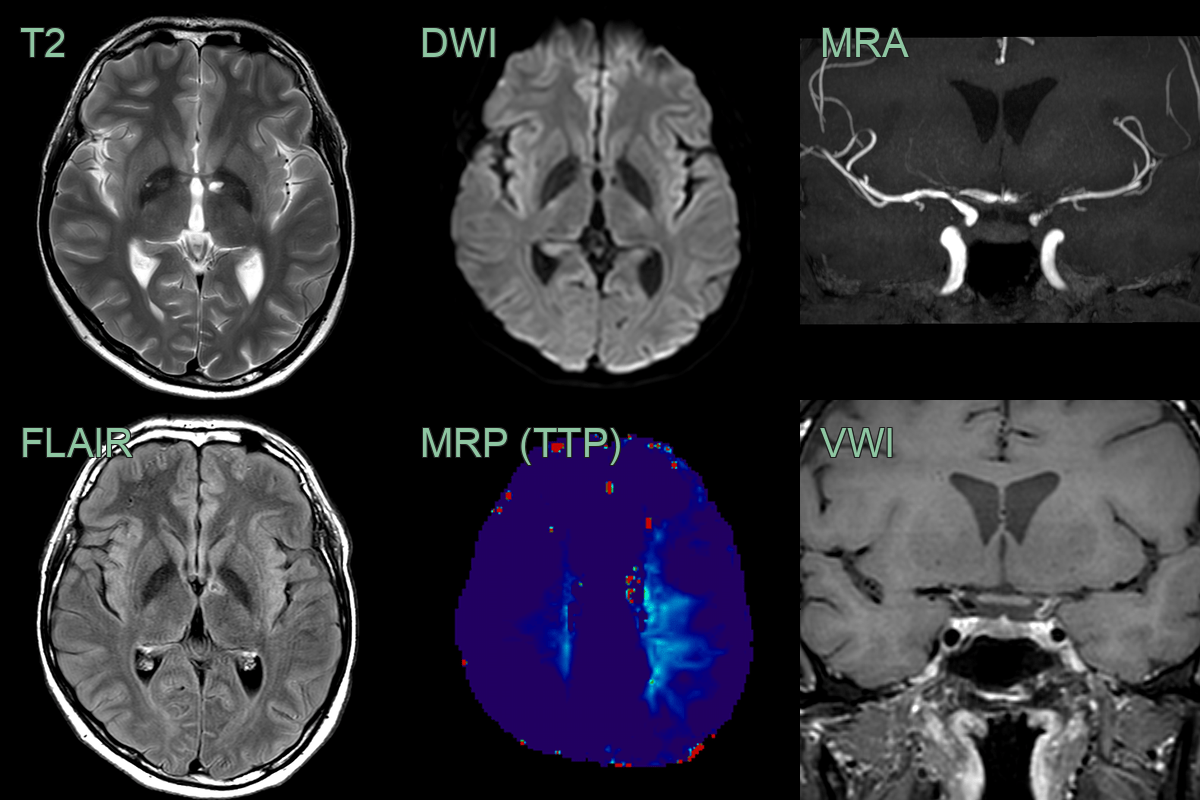
- A 35-year-old patient presenting with photophobia and headache was diagnosed with HIV with a CD40 count of 80.
- Baseline MRI showed an old infarct in the left thalamus. VWI imaging showed concentric enhancement within stenosis in the terminal ICA and MCA.
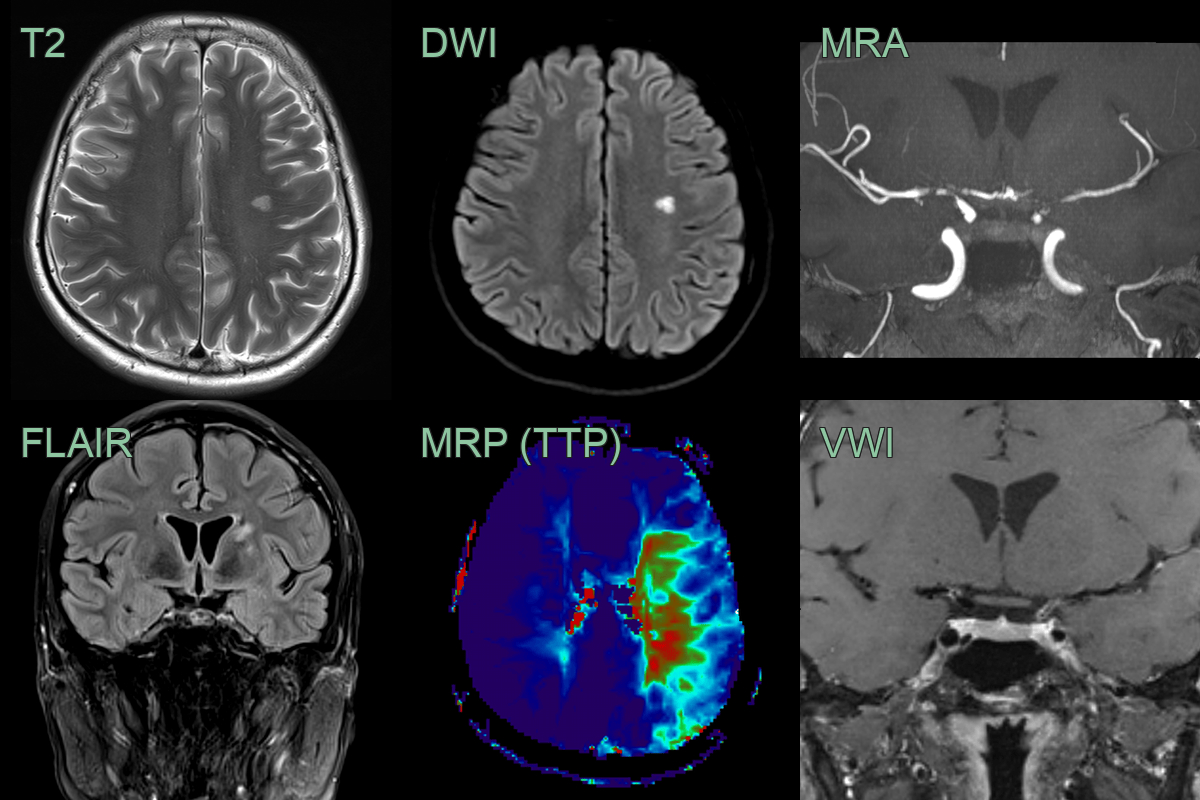
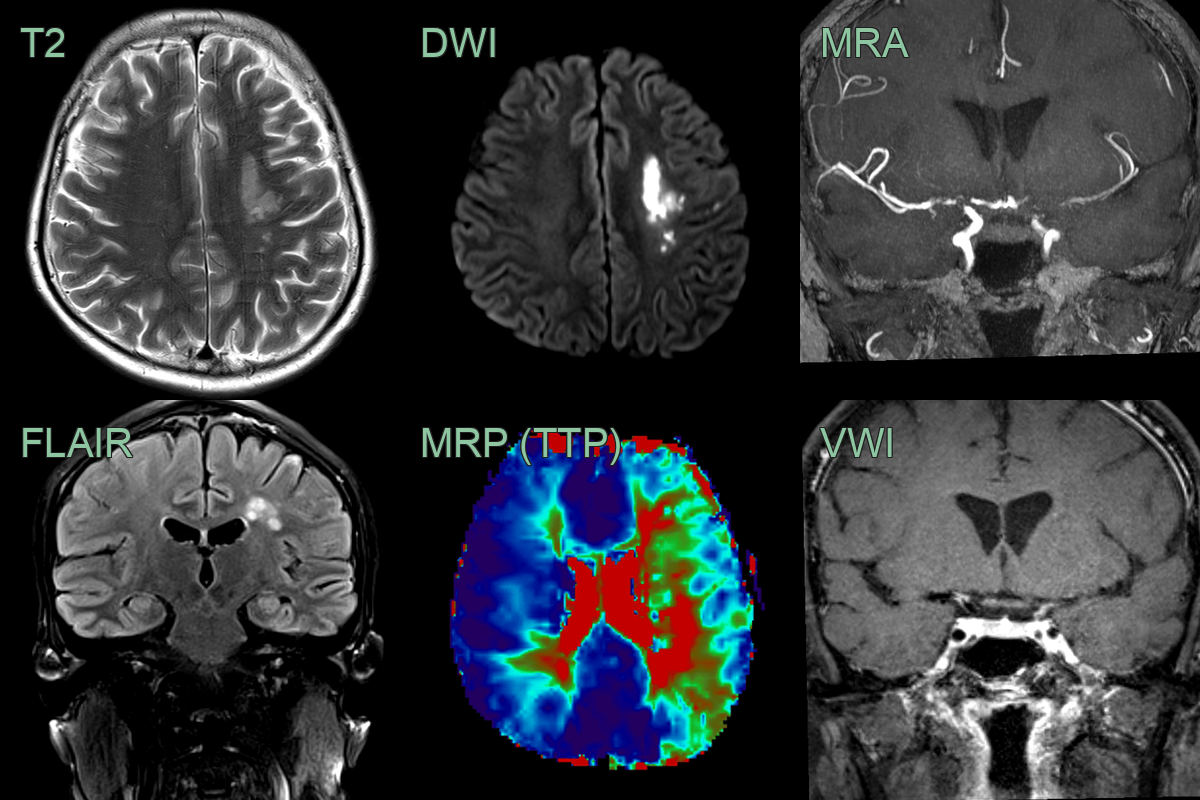
- Over the following 4-6 weeks, the mural enhancement was static. The stenoses only minimally progressed but the perfusion to the left and, to a lesser extent, right cerebral hemisphere worsened.
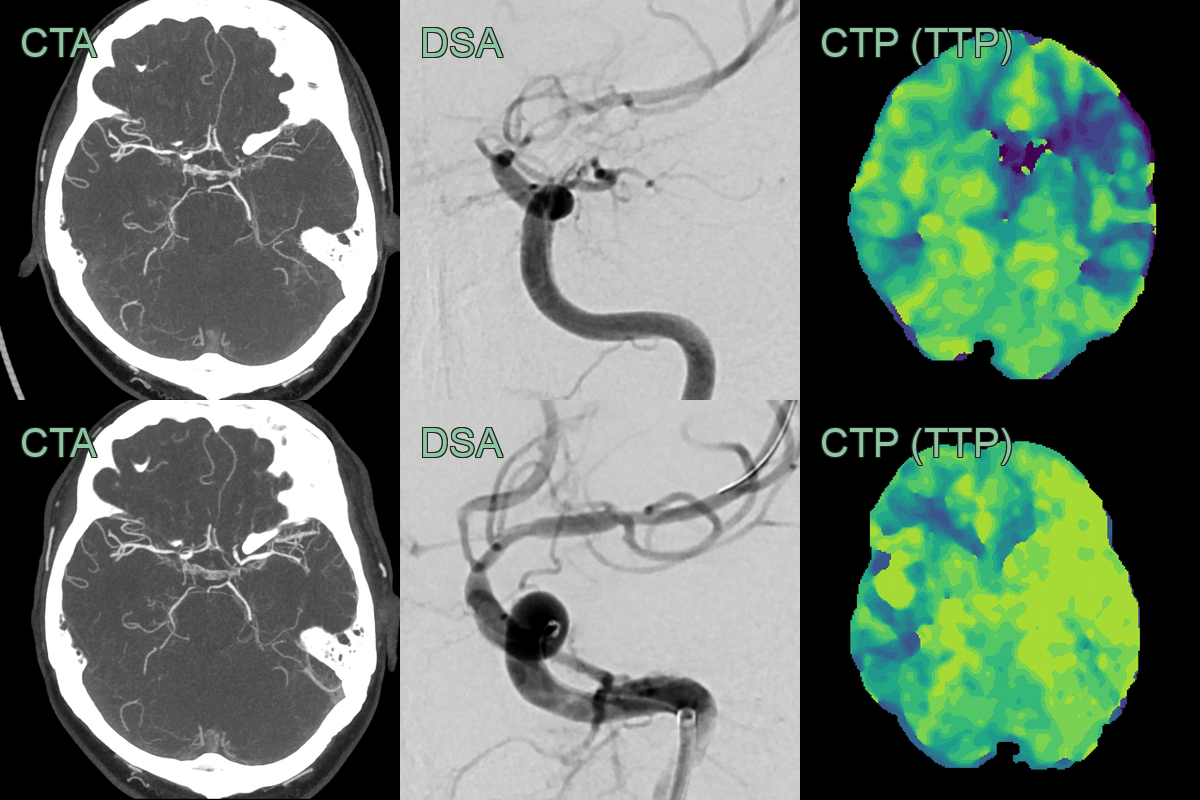
- With worsening perfusion, an angioplasty successfully widened the stenosis and significantly improved perfusion.
Treatment¶
- Goals: suppress inflammation, prevent organ damage, and manage complications
- Corticosteroids: mainstay of initial treatment for most types
- Immunosuppressive agents:
- Cyclophosphamide, methotrexate, azathioprine
- Rituximab for ANCA-associated vasculitis
- Biological agents:
- TNF inhibitors (e.g. infliximab) for refractory cases
- Tocilizumab for giant cell arteritis
- Antiplatelet therapy: to reduce risk of thrombotic complications
- Surgical intervention:
- Aneurysm repair
- Revascularisation for severe stenosis
- Regular imaging follow-up to assess treatment response and detect complications
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Reversible cerebral vasoconstriction syndrome (RCVS) | Multifocal segmental arterial narrowing that resolves on follow-up MRA within 12 weeks; no vessel wall enhancement on high-resolution MRI |
| Moyamoya disease | Bilateral ICA terminus and proximal MCA/ACA stenosis with "puff of smoke" lenticulostriate collaterals on DSA; no small vessel beading |
| Atherosclerosis | Calcified eccentric plaques on CTA; diffuse large vessel involvement; no small vessel beading pattern |
| Fibromuscular dysplasia | "String of beads" alternating narrowing and dilatation primarily in renal and cervical arteries; no intracranial small vessel involvement |
| Sarcoidosis | Leptomeningeal and perivascular enhancement; cranial nerve involvement; vessel narrowing from periarterial inflammation; hilar lymphadenopathy on chest CT |
| Takayasu arteritis | Concentric vessel wall thickening and enhancement of large arteries on MRI/CTA; no intracranial small vessel involvement; predominantly extracranial |