Ventral Cord Herniation¶
Summary
- Rare condition characterised by anterior herniation of the spinal cord through a dural defect, most commonly occurring in the thoracic spine
- Presents with progressive myelopathy, often with Brown-Séquard-like syndrome or asymmetric motor and sensory deficits
- MRI demonstrates focal anterior displacement of the cord with characteristic "C-shaped" configuration on axial images and obliteration of the anterior CSF space
Pathophysiology¶
- Etiology remains unclear with multiple proposed mechanisms:
- Congenital dural defect theory
- Acquired defect from trauma, inflammation, or disc herniation erosion
- CSF pressure gradients causing progressive herniation
- Pathologic process:
- Ventral dural defect allows cord herniation
- Tethering and strangulation of cord at defect edges
- Progressive myelopathy from chronic compression and ischaemia
- Associated adhesions between cord and ventral dura
- Classification:
- Type K: focal herniation with kink/angulation
- Type D: diffuse smooth ventral displacement
- Type P: associated with ventral pseudomeningocele
Demographics¶
- Incidence:
- Extremely rare condition
- Less than 200 cases reported in literature
- Age:
- Middle-aged adults (40-60 years)
- Mean age at diagnosis: 50 years
- Gender:
- Female predominance (F:M ratio approximately 2:1)
- Location:
- Mid-thoracic spine most common (T3-T7)
- Rarely cervical or lumbar
Diagnosis¶
- Clinical presentation:
- Insidious onset of progressive myelopathy
- Brown-Séquard syndrome (most common)
- Asymmetric motor weakness
- Sensory level deficit
- Spasticity and hyperreflexia below lesion
- Bowel/bladder dysfunction (late finding)
- Physical examination:
- Upper motor neuron signs
- Asymmetric weakness
- Dissociated sensory loss
- Positive Babinski sign
- Differential diagnosis:
- Arachnoid cyst
- Intradural disc herniation
- Spinal cord tumour
- Transverse myelitis
- Anterior spinal artery syndrome
Imaging¶
- MRI (modality of choice):
- T2:
- Focal anterior displacement of spinal cord
- "C-shaped" or "boomerang" configuration on axial images
- Obliteration of anterior subarachnoid space
- Possible cord signal hyperintensity (myelomalacia/oedema)
- Widened dorsal subarachnoid space
- T1:
- Anterior displacement of cord
- Loss of normal anterior CSF signal
- Cord may appear adherent to vertebral body
- T1+C:
- No enhancement typically
- May show enhancement if associated inflammation
- Sagittal imaging:
- Focal kink or angulation of cord
- "Scalpel sign" - sharp ventral indentation
- Axial imaging:
- Characteristic C-shaped cord configuration
- Cord adherent to posterior vertebral body/disc
- CISS/FIESTA sequences:
- Better delineation of dural defect
- Improved visualization of arachnoid adhesions
- CT Myelography:
- Historical importance, largely replaced by MRI
- Shows ventral filling defect
- Cord displacement anteriorly
- May demonstrate dural defect
- Plain radiographs:
- Usually normal
- May show associated spinal deformity
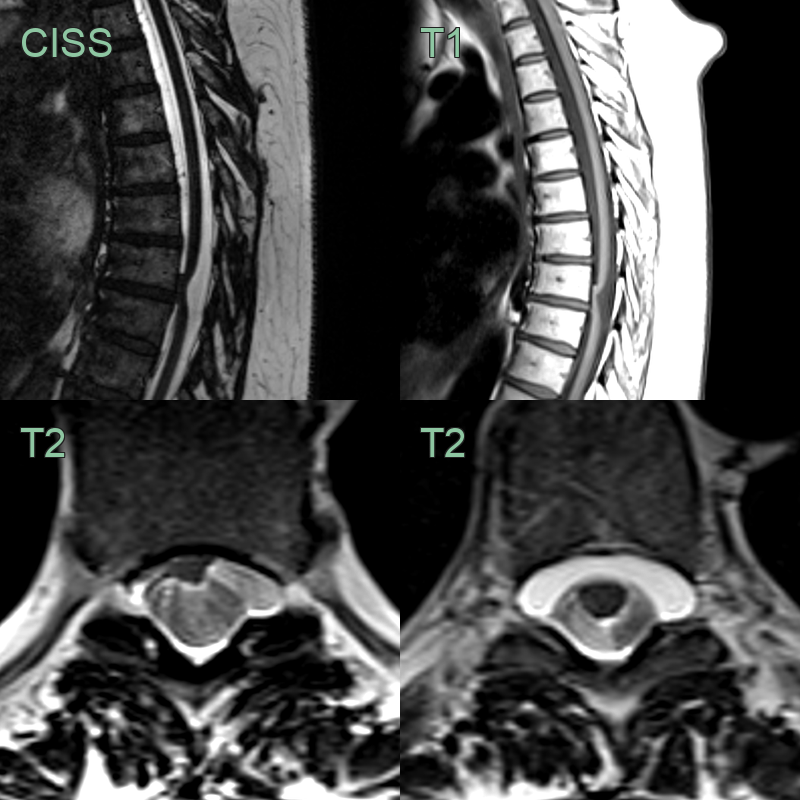
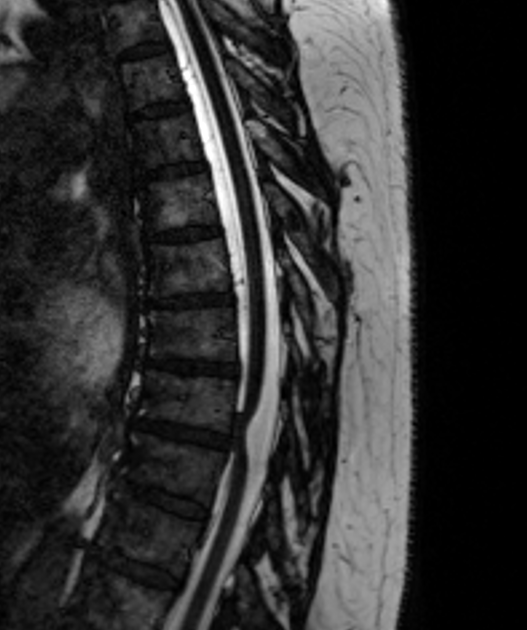
- A 45-year-old patient experienced a long progressive history of numbness and mild weakness in both legs.
- MRI showed the cord displaced anteriorly against the ventral theca.
- There was also a ventral epidural collections indicating a CSF leak and hernation of the cord into the defect.
Treatment¶
- Conservative management:
- Observation for mild/stable symptoms
- Physical therapy
- Pain management
- Regular clinical and imaging follow-up
- Surgical intervention:
- Indications:
- Progressive neurological deficit
- Significant myelopathy
- Disabling symptoms
- Surgical techniques:
- Posterior approach with laminectomy -
Differential diagnosis¶
| Differential diagnosis | Differentiating feature |
|---|---|
| Arachnoid cyst | Cyst appears as CSF-filled space posterior to cord; cord displaced anteriorly rather than herniated through dura |
| Spinal cord infarction | Acute onset of symptoms; T2 hyperintensity within cord parenchyma; no anterior displacement or herniation |
| Multiple sclerosis | Multiple lesions in space and time; plaques within cord substance rather than herniation; brain lesions often present |
| Syringomyelia | Fluid-filled cavity within the cord parenchyma; cord may be expanded rather than herniated |
| Spinal arteriovenous malformation/fistula | Flow voids on MRI; serpentine vessels along cord surface; cord oedema without herniation |
| Spinal cord tumour | Mass effect with cord expansion; enhancement with contrast; no ventral herniation through dural defect |
| Transverse myelitis | Acute inflammatory process; long segment T2 hyperintensity; cord swelling without herniation |
| Spinal cord atrophy | Diffuse cord thinning without focal anterior displacement; no dural defect |
| Epidural lipomatosis | Excessive epidural fat causing cord compression; no dural defect or cord herniation |
| Disc herniation with cord compression | Disc material visible; cord compressed posteriorly rather than herniated anteriorly |