Vertebral Artery Dissection¶
Summary
- Vertebral artery dissection (VAD) is a tear in the inner lining of the vertebral artery, leading to intramural haematoma formation
- Presents with neck pain, headache, and posterior circulation ischaemic symptoms
- Diagnosis relies on clinical presentation and neuroimaging findings
Pathophysiology¶
- Intimal tear allows blood to enter the arterial wall, creating a false lumen
- Mechanisms:
- Spontaneous: often associated with connective tissue disorders
- Traumatic: minor trauma or sudden neck movements
- Consequences:
- Luminal stenosis or occlusion
- Thrombus formation and distal embolisation
- Subarachnoid haemorrhage (rare)
Demographics¶
- Incidence: 1-1.5 per 100,000 per year
- Age: typically affects young to middle-aged adults (mean age 40-45 years)
- Gender: slight female predominance
- Risk factors:
- Hypertension
- Smoking
- Migraine
- Oral contraceptive use
- Connective tissue disorders (e.g., Ehlers-Danlos syndrome, Marfan syndrome)
Diagnosis¶
- Clinical presentation:
- Neck pain or occipital headache (often unilateral)
- Posterior circulation ischaemic symptoms:
- Vertigo
- Diplopia
- Ataxia
- Lateral medullary syndrome (Wallenberg syndrome)
- Physical examination:
- Horner's syndrome (ipsilateral miosis, ptosis, and anhidrosis)
- Nystagmus
- Cerebellar signs
- Laboratory tests:
- No specific blood markers for VAD
- Consider testing for connective tissue disorders if suspected
Imaging¶
- CT angiography (CTA):
- First-line imaging modality
- Findings:
- Eccentric luminal narrowing
- Intramural haematoma (crescent sign)
- Vessel irregularity or pseudoaneurysm formation
- MRI and MR angiography (MRA):
- Superior soft tissue contrast
- Findings:
- Intramural haematoma: hyperintense on T1-weighted fat-suppressed images
- Luminal narrowing or occlusion on MRA
- Digital subtraction angiography (DSA):
- Gold standard for diagnosis
- Reserved for cases with equivocal non-invasive imaging or when endovascular treatment is planned
- Findings:
- String sign (long, irregular narrowing)
- Pearl-and-string sign (alternating dilatations and stenoses)
- Pseudoaneurysm formation
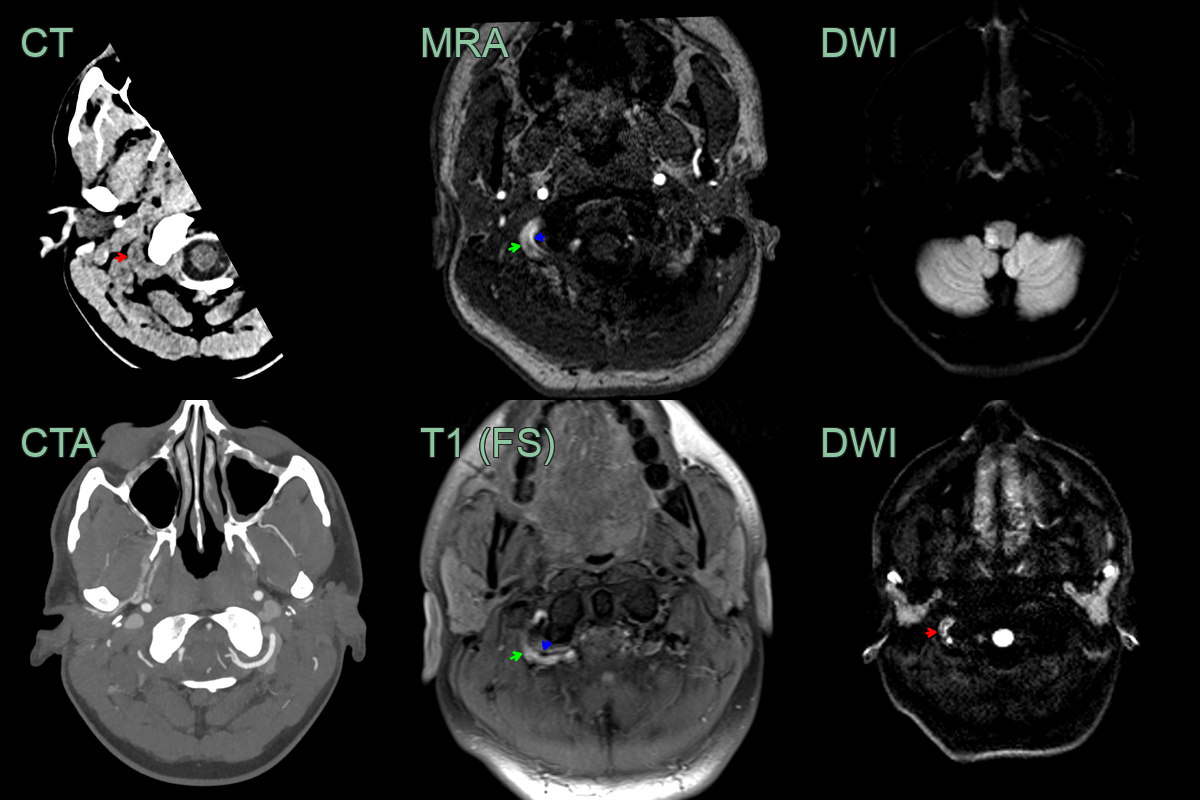
- A 30 year patient presented with dizziness, nystagmus, dysphagia and ataxia.
- CT showed a subtly hyperdense rim around the left V3 vertebral artery (red arrow).
- The corresponded thrombus causing DWI hyperintensity (red arrow) and T1-shortening on the ToF angiogram (red arrow) next to flow-related signal from the narrowed lumen (blue arrow).
- The Wallenberg syndrome) was caused by a lateral medullary infarct.
Treatment¶
- Acute management:
- Antithrombotic therapy:
- Anticoagulation (heparin followed by warfarin) for 3-6 months
- Antiplatelet therapy (aspirin) as an alternative
- Pain management
- Blood pressure control
- Endovascular treatment:
- Indicated for persistent symptoms despite medical management or expanding pseudoaneurysms
- Options:
- Stenting
- Coil embolisation for pseudoaneurysms
- Surgical intervention:
- Rarely required
- Considered for persistent symptoms or recurrent dissections
- Secondary prevention:
- Long-term antiplatelet therapy
- Lifestyle modifications (smoking cessation, blood pressure control)
- Avoidance of activities with sudden neck movements